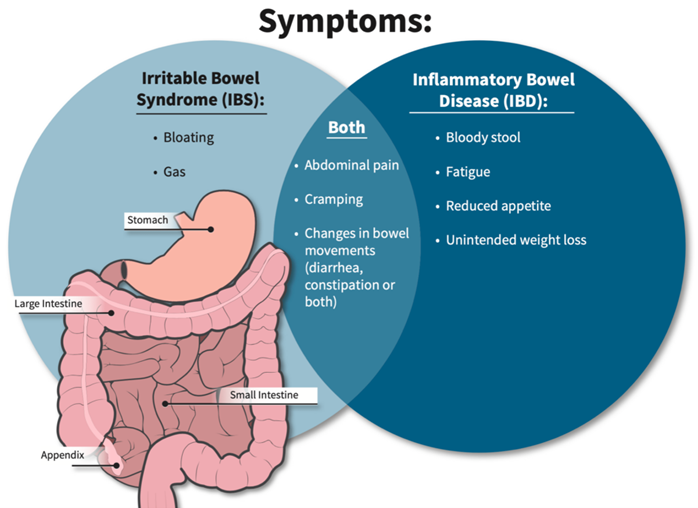
A nurse provides education to a client diagnosed with inflammatory bowel syndrome (IBS) about measures to treat diarrhea caused by acute flare-ups. Which statement by the client indicates a need for further teaching?
"I will eat frequent small meals."
"I will increase the intake of leafy greens and other sources of dietary fiber."
"I will increase fluids."
"I will take prescribed medications on schedule to regulate bowel patterns."
The Correct Answer is B
Choice A reason: This is correct because eating frequent small meals can help the client with IBS to avoid overloading the digestive system and triggering diarrhea. The nurse should advise the client to eat slowly chew well, and avoid foods that are spicy, fatty, or gas-producing.
Choice B reason: This is incorrect because increasing the intake of leafy greens and other sources of dietary fiber can worsen diarrhea by increasing stool bulk and motility. The nurse should advise the client to limit or avoid high-fiber foods, such as whole grains, fruits, vegetables, nuts, and seeds, during acute flare-ups of IBS. The client can gradually reintroduce fiber when the symptoms subside.
Choice C reason: This is correct because increasing fluids can help the client with IBS to prevent dehydration and electrolyte imbalance caused by diarrhea. The nurse should advise the client to drink at least 8 glasses of water per day and avoid caffeinated, alcoholic, or carbonated beverages that can irritate the bowel or cause gas.
Choice D reason: This is correct because taking prescribed medications on schedule can help the client with IBS to regulate bowel patterns and reduce diarrhea. The nurse should instruct the client on how to use medications, such as antidiarrheals, antispasmodics, or probiotics, as ordered by the provider. The nurse should also monitor the client for any adverse effects or interactions of the medications.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Choice A Reason: This choice is incorrect. Inability to perform within normal limits is a vague and general term that does not describe the specific finding of left facial droop. The nurse should document the exact observation and compare it to the expected or normal range.
Choice B Reason: This choice is incorrect. Symmetrical findings mean that both sides of the body or face are equal or similar in appearance or function. Left facial droop indicates that one side of the face is lower or weaker than the other, which is not symmetrical.
Choice C Reason: This is the correct choice. Asymmetrical findings mean that both sides of the body or face are unequal or different in appearance or function. Left facial droop indicates that one side of the face is lower or weaker than the other, which is asymmetrical.
Choice D Reason: This choice is incorrect. Bilateral strength present means that both sides of the body or face have normal or adequate muscle power or force. Left facial droop indicates that one side of the face has reduced or impaired muscle power or force, which is not bilateral strength present.
Correct Answer is D
Explanation
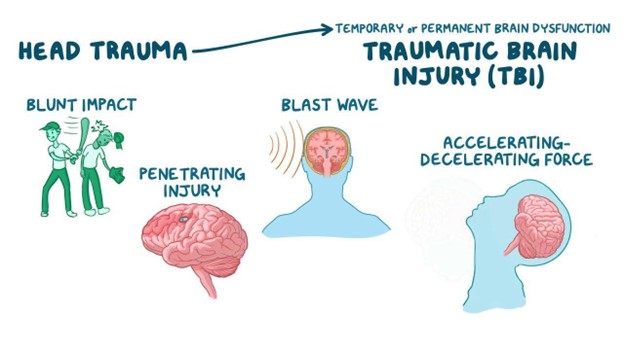
Choice A Reason: This is incorrect because nystagmus is not a response to stimuli, but a condition that causes involuntary eye movements. Nystagmus can be caused by various factors, such as inner ear disorders, brain lesions, or drug toxicity, but not necessarily by cervical spine injury.
Choice B Reason: This is incorrect because decorticate positioning is a response to stimuli that indicates damage to the cerebral cortex or the corticospinal tract. Decorticate positioning is characterized by flexion of the arms and extension of the legs. It does not indicate cervical spine injury, which affects the spinal cord below the brainstem.
Choice C Reason: This is incorrect because lack of any response to stimuli can indicate various levels of brain damage or coma, but not specifically cervical spine injury. Lack of any response can also be influenced by other factors, such as sedation, hypothermia, or shock.
Choice D Reason: This is correct because decerebrate positioning is a response to stimuli that indicates damage to the brainstem or the upper cervical spine. Decerebrate positioning is characterized by extension and outward rotation of the arms and legs. It indicates a severe and life-threatening injury that can impair vital functions, such as breathing and blood pressure.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today