A nurse in an ophthalmology clinic is interviewing a client who was referred by his primary care provider for suspicion of cataracts. Which of the following findings is consistent with manifestations of cataracts?
Loss of peripheral vision
A decreased ability to perceive colors
Loss of central vision
Seeing bright flashes of light and floaters
The Correct Answer is B
Choice A reason: This is incorrect because loss of peripheral vision is not a manifestation of cataracts, but of glaucoma. Glaucoma is a condition that causes increased pressure inside the eye and damage to the optic nerve, which can lead to loss of vision in the outer edges of the visual field. The nurse should assess the client's intraocular pressure and visual field test results to rule out glaucoma.
Choice B reason: This is correct because a decreased ability to perceive colors is a manifestation of cataracts. Cataracts are a condition that causes clouding or opacity of the lens, which is the transparent structure behind the pupil that focuses light onto the retina. Cataracts can reduce the clarity and contrast of vision and make colors appear faded or yellowish. The nurse should ask the client about any changes in color perception or brightness of objects.
Choice C reason: This is incorrect because loss of central vision is not a manifestation of cataracts but of macular degeneration. Macular degeneration is a condition that affects the macula, which is the central part of the retina that is responsible for sharp and detailed vision. Macular degeneration can cause blurred or distorted central vision, difficulty reading or recognizing faces, or dark spots in the visual field. The nurse should assess the client's visual acuity and fundoscopic examination results to rule out macular degeneration.
Choice D reason: This is incorrect because seeing bright flashes of light and floaters is not a manifestation of cataracts but of retinal detachment. Retinal detachment is a condition that occurs when the retina, which is the layer of tissue at the back of the eye that converts light into nerve impulses, separates from its underlying support tissue. Retinal detachment can cause sudden flashes of light, floaters, or shadows in the visual field. The nurse should refer the client to an ophthalmologist immediately if retinal detachment is suspected.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is ["A","B","E"]
Explanation
Choice A Reason: This is a correct choice. Trying to avoid scratching is an advice that the nurse will provide to the client, as it prevents further damage and infection of the skin. Scratching can break the skin barrier and introduce bacteria or fungi into the wound, leading to inflammation and complications.
Choice B Reason: This is a correct choice. Applying a moist cool compress is an advice that the nurse will provide to the client, as it soothes and relieves itching and swelling. A moist cool compress can reduce inflammation and histamine release, which are responsible for allergic symptoms.
Choice C Reason: This is an incorrect choice. Using alcohol to cleanse the area is not an advice that the nurse will provide to the client, as it irritates and dries out the skin. Alcohol can strip away the natural oils and moisture from the skin, making it more prone to cracking and itching.
Choice D Reason: This is an incorrect choice. Using a wooden stick to scratch lesions is not an advice that the nurse will provide to the client, as it causes more harm than good. A wooden stick can injure or infect the skin, as well as spread the allergen or irritant to other areas.
Choice E Reason: This is a correct choice. Avoiding hot air is an advice that the nurse will provide to the client, as it aggravates itching and inflammation. Hot air can increase blood flow and histamine release, which are responsible for allergic symptoms. The client should also avoid hot water or showers, as they can have the same effect.
Correct Answer is A
Explanation
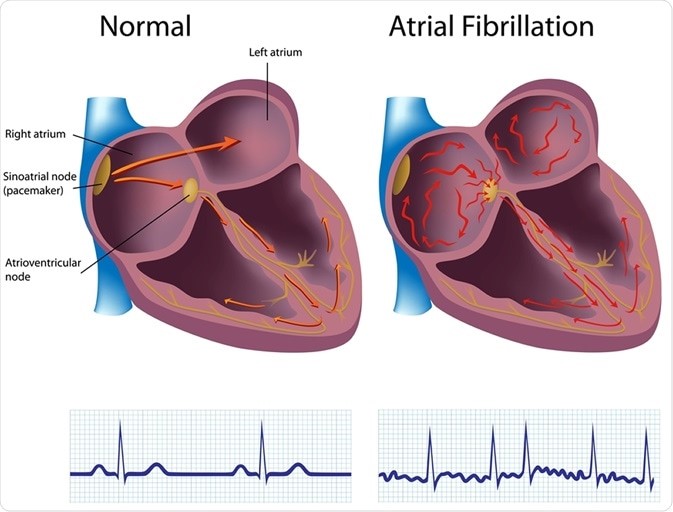
Choice A reason: This is the correct answer because atrial fibrillation is the risk factor that puts the client at
the highest risk for embolic stroke. Atrial fibrillation is an irregular and rapid heart rate that causes poor blood flow and blood pooling in the heart chambers. This can lead to the formation of blood clots that can travel to the brain and block an artery, causing an embolic stroke.
Choice B reason: This is incorrect because hypertension is not the risk factor that puts the client at
the highest risk for embolic stroke. Hypertension is high blood pressure that puts stress on the blood vessels and increases the risk of bleeding or rupture. This can lead to a hemorrhagic stroke, but not an embolic stroke.
Choice C reason: This is incorrect because diabetes is not the risk factor that puts the client at
the highest risk for embolic stroke. Diabetes is a condition that causes high blood sugar levels and damages the blood vessels and nerves. This can lead to poor circulation and increased risk of infection and ulcers, but not an embolic stroke.
Choice D reason: This is incorrect because alcohol abuse is not the risk factor that puts the client at
the highest risk for embolic stroke. Alcohol abuse is excessive consumption of alcohol that affects liver function and blood clotting factors. This can lead to liver disease and bleeding disorders, but not an embolic stroke.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today