After completing a neurological assessment, the nurse documents that the client is stuporous. Which of the following describes this level of consciousness?
Minimal movement, verbal responses limited to sounds, awakens briefly only with extreme vigorous stimulation.
Extremely drowsy, minimally responsive, limited ability to follow commands, vigorous stimulation needed to waken.
Alert and oriented x3, sluggish, drowsy, wakes to voice or gentle shaking.
Does not respond to verbal stimuli, does not speak, decorticate/decerebrate posturing in response to pain.
The Correct Answer is A
Choice A reason: This is the correct answer because this describes a stupor, which is a state of near-unconsciousness or reduced responsiveness. A stuporous client shows minimal movement and verbal responses and requires extreme vigorous stimulation such as painful stimuli to awaken briefly.
Choice B reason: This is incorrect because this describes obtundation, which is a state of reduced alertness or awareness. An obtunded client is extremely drowsy and minimally responsive and requires vigorous stimulation such as shaking or shouting to wake.
Choice C reason: This is incorrect because this describes lethargy, which is a state of decreased energy or activity. A lethargic client is alert and oriented x3 (to person, place, and time), but sluggish and drowsy, and wakes to voice or gentle shaking.
Choice D reason: This is incorrect because this describes a coma, which is a state of deep unconsciousness or unresponsiveness. A comatose client does not respond to verbal stimuli or speak and shows abnormal posturing in response to pain, such as decorticate (flexion of arms and extension of legs) or decerebrate (extension of arms and legs).
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
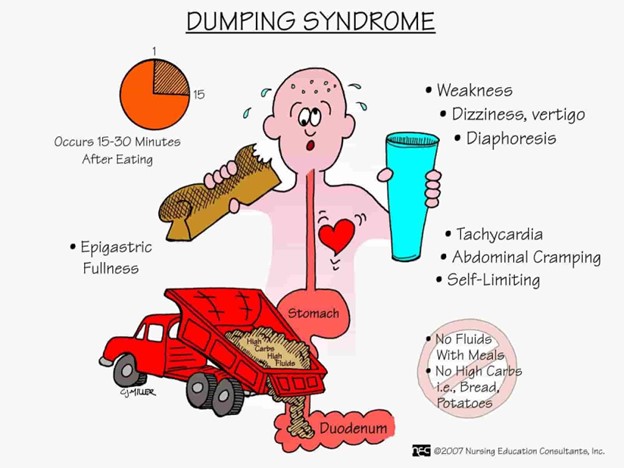
Choice A Reason: Sweating and pallor are early signs and symptoms of dumping syndrome, which is a condition where food moves too quickly from the stomach to the small intestine, causing rapid fluid shifts and hormonal changes. Sweating and pallor are caused by hypoglycemia, which occurs when the high concentration of food in the small intestine stimulates insulin secretion.
Choice B Reason: Abdominal cramping and pain are late signs and symptoms of dumping syndrome, which occur about one to three hours after eating. Abdominal cramping and pain are caused by intestinal distension, spasms, and gas formation.
Choice C Reason: Double vision and chest pain are not signs and symptoms of dumping syndrome, but may indicate other serious conditions, such as stroke or heart attack. Double vision and chest pain should be reported to the provider immediately.
Choice D Reason: Bradycardia and indigestion are not signs and symptoms of dumping syndrome, but may be related to other gastrointestinal disorders, such as gastritis or peptic ulcer disease. Bradycardia and indigestion should be evaluated by the provider for further diagnosis and treatment.
Correct Answer is B
Explanation
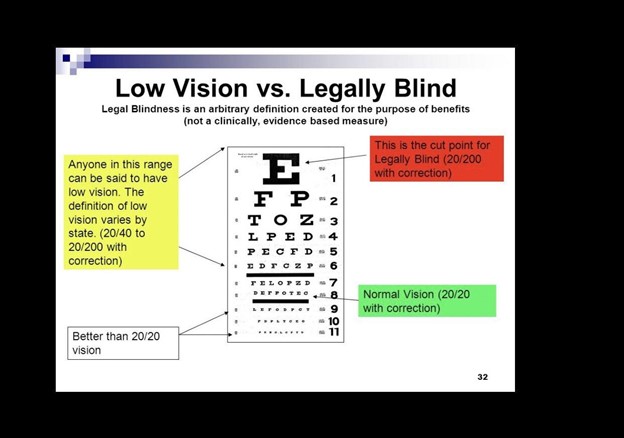
Choice A Reason: This is incorrect because full vision loss in one eye does not necessarily mean that the person is legally blind. Legal blindness depends on the visual acuity and visual field of both eyes.
Choice B Reason: This is correct because legal blindness is defined by the World Health Organization (WHO) as having a visual acuity of 20/200 or worse in the better eye with the best possible correction, such as glasses or contact lenses. This means that the person can see at 20 feet what a normal person can see at 200 feet.
Choice C Reason: This is incorrect because inability to see clearly from 200 feet away without corrective lenses may indicate nearsightedness or myopia, but not legal blindness. Nearsightedness can be corrected with lenses or surgery.
Choice D Reason: This is incorrect because bilateral visual impairment of 20/60 or greater does not meet the criteria for legal blindness. Visual impairment is defined by WHO as having a visual acuity of less than 20/60 but better than 20/200 in the better eye with the best possible correction.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today