A client's chart indicates that they are legally blind. Which of the following is the definition of legally blind?
Full vision loss in at least one eye
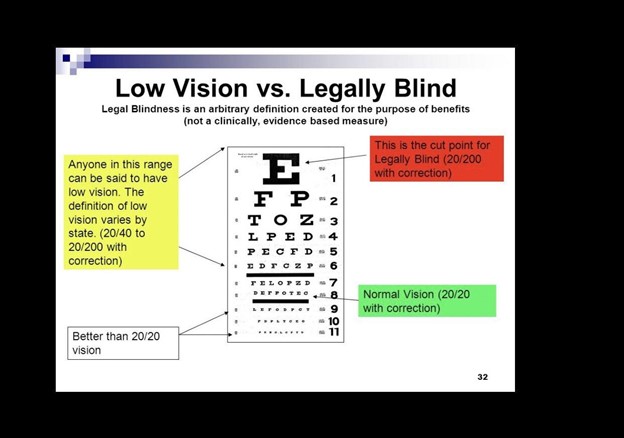
The best-corrected vision in the better eye of 20/200 or less
Inability to see clearly from 200 feet away without corrective lenses
Bilateral visual impairment of 20/60 or greater
The Correct Answer is B
Choice A Reason: This is incorrect because full vision loss in one eye does not necessarily mean that the person is legally blind. Legal blindness depends on the visual acuity and visual field of both eyes.
Choice B Reason: This is correct because legal blindness is defined by the World Health Organization (WHO) as having a visual acuity of 20/200 or worse in the better eye with the best possible correction, such as glasses or contact lenses. This means that the person can see at 20 feet what a normal person can see at 200 feet.
Choice C Reason: This is incorrect because inability to see clearly from 200 feet away without corrective lenses may indicate nearsightedness or myopia, but not legal blindness. Nearsightedness can be corrected with lenses or surgery.
Choice D Reason: This is incorrect because bilateral visual impairment of 20/60 or greater does not meet the criteria for legal blindness. Visual impairment is defined by WHO as having a visual acuity of less than 20/60 but better than 20/200 in the better eye with the best possible correction.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Choice A Reason: Requesting the charge nurse put the client on the surgery schedule is not the best first action, as it does not address the urgency of the situation. The client may have a perforated appendix, which is a life-threatening complication that requires immediate intervention.
Choice B Reason: Documenting the WBC count from the morning labs is not the best first action, as it does not address the client's current condition. The WBC count may be elevated due to inflammation or infection, but it does not indicate the severity of the problem.
Choice C Reason: This is the correct choice. Notifying the healthcare provider is the best first action, as it alerts them to the possibility of a perforated appendix and allows them to order appropriate tests and treatments.
Choice D Reason: Providing an antiemetic is not the best first action, as it does not address the underlying cause of the vomiting. The client may have peritonitis, which is inflammation of the abdominal cavity due to leakage of intestinal contents. An antiemetic may mask this symptom and delay diagnosis and treatment.
Correct Answer is A
Explanation
Choice A Reason: The client needs total nursing care is the expected outcome for a client who has a score of 6 on the Glasgow Coma Scale, which is a tool that measures the level of consciousness based on eye opening, verbal response, and motor response. A score of 6 indicates severe brain injury and coma, meaning that the client is unresponsive and dependent on others for all activities of daily living.
Choice B Reason: Indicates stable neurologic status is not the expected outcome for a client who has a score of 6 on the Glasgow Coma Scale, which indicates severe brain injury and coma. A stable neurologic status means that there are no changes in the level of consciousness, vital signs, or neurological signs.
Choice C Reason: The client has a decline in level of consciousness but is able to protect his airway is not the expected outcome for a client who has a score of 6 on the Glasgow Coma Scale, which indicates severe brain injury and coma. A decline in level of consciousness means that the client is less alert and responsive than normal, but still able to respond to stimuli and maintain airway patency.
Choice D Reason: The client is alert and oriented is not the expected outcome for a client who has a score of 6 on the Glasgow Coma Scale, which indicates severe brain injury and coma. Alert and oriented means that the client is fully awake and aware of person, place, time, and situation.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today