While assessing the newborn, the nurse should be aware that the average expected apical pulse range of a full-term, quiet, alert newborn is __ beats/min.
100 to 120
120 to 160
80 to 100
150 to 180
The Correct Answer is B
Choice a) 100 to 120 is incorrect because this is too low for a normal newborn's heart rate. The heart rate of a newborn is influenced by factors such as gestational age, activity level, temperature, and health status. A full-term, quiet, alert newborn should have a heart rate between 120 and 160 beats per minute, which reflects their high metabolic rate and oxygen demand. A heart rate below 100 beats per minute may indicate bradycardia, which can be caused by hypoxia, hypothermia, or cardiac problems.
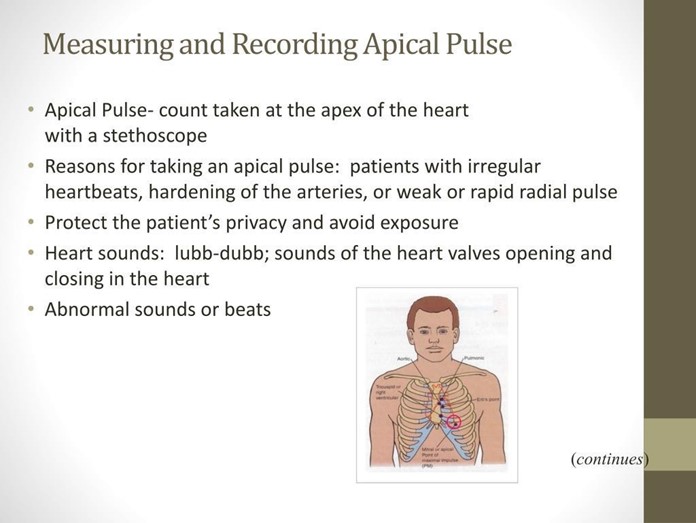
Choice b) 120 to 160 is correct because this is the normal range for a full-term, quiet, alert newborn's heart rate. The apical pulse is the best way to measure the heart rate of a newborn, as it reflects the actual contractions of the heart. The apical pulse can be auscultated at the fourth intercostal space on the left side of the chest, just below the nipple line. The nurse should count the apical pulse for a full minute, as it may vary with the respiratory cycle.
Choice c) 80 to 100 is incorrect because this is also too low for a normal newborn's heart rate. A full-term, quiet, alert newborn should have a heart rate between 120 and 160 beats per minute, which is higher than that of an adult or an older child. A heart rate below 100 beats per minute may indicate bradycardia, which can be caused by hypoxia, hypothermia, or cardiac problems.
Choice d) 150 to 180 is incorrect because this is too high for a normal newborn's heart rate. A full-term, quiet, alert newborn should have a heart rate between 120 and 160 beats per minute, which is lower than that of a preterm or a crying newborn. A heart rate above 160 beats per minute may indicate tachycardia, which can be caused by fever, infection, anemia, or hyperthyroidism.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
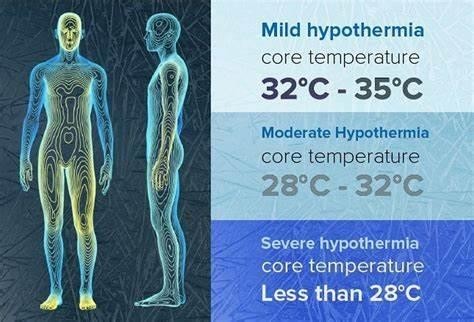
Choice A) Decreased metabolic rate is incorrect because this is not a result of hypothermia in the newborn, but rather a cause of it. Metabolic rate is the speed at which the body uses energy to perform its functions. Newborns have a high metabolic rate, which helps them to maintain a normal body temperature of 36.5°C to 37.5°C (97.7°F to 99.5°F). However, some factors can lower the metabolic rate of newborns, such as prematurity, low birth weight, infection, or hypoglycemia. A low metabolic rate can make the newborn more susceptible to heat loss and hypothermia, which is a condition that occurs when the body temperature drops below 36°C (96.8°F). Therefore, this response is inaccurate and misleading.
Choice B) Decreased oxygen demands is incorrect because this is not a result of hypothermia in the newborn, but rather a consequence of it. Oxygen demand is the amount of oxygen that the body needs to function properly.
Newborns have a high oxygen demand, which helps them to support their growth and development. However, some factors can decrease the oxygen demand of newborns, such as hypothermia, sedation, or asphyxia. A low oxygen demand can impair the oxygen delivery and utilization by the tissues and organs, leading to hypoxia, acidosis, or organ failure. Therefore, this response is irrelevant and inaccurate.
Choice C) Shivering to generate heat is incorrect because this is not a result of hypothermia in the newborn, but rather a mechanism that is absent in them. Shivering is an involuntary contraction of the muscles that produces heat and raises the body temperature. It is a common response to cold exposure in adults and older children, but not in newborns. Newborns do not have the ability to shiver, as their muscles are immature and lack glycogen stores.
Instead, they rely on other methods to generate heat, such as non-shivering thermogenesis, which involves burning brown fat in certain areas of the body. Therefore, this response is irrelevant and inaccurate.
Choice D) Increased glucose demands is correct because this is a result of hypothermia in the newborn that can cause complications. Glucose demand is the amount of glucose that the body needs to produce energy and maintain its functions. Newborns have a high glucose demand, which helps them to support their metabolic rate and thermoregulation. However, some factors can increase the glucose demand of newborns, such as hypothermia, stress, or infection. A high glucose demand can deplete the glucose stores and cause hypoglycemia, which is a low level of glucose in the blood that can lead to seizures, brain damage, or death. Therefore, this response is clear and accurate.
Correct Answer is C
Explanation
Choice a) Breasts firm and tender is incorrect because this is not a sign of normal involution, but rather a sign of breast engorgement, which is a common problem in the first few weeks of breastfeeding. Breast engorgement occurs when thE breasts become overfilled with milk, causing them to feel hard, swollen, painful, and warm. It can be prevented or relieved by frequent and effective breastfeeding, applying warm or cold compresses, massaging the breasts, expressing some milk, and wearing a supportive bra.
Choice b) Episiotomy slightly red and puffy is incorrect because this is not a sign of normal involution, but rather a sign of inflammation or infection of the perineal wound. An episiotomy is a surgical cut made in the perineum (the area between the vagina and the anus) to enlarge the vaginal opening during delivery. It can take several weeks to heal and may cause pain, swelling, bruising, bleeding, or discharge. It can be cared for by keeping the area clean and dry, applying ice packs or witch hazel pads, taking painkillers or sitz baths, and avoiding constipation or straining.
Choice c) Fundus below the symphysis and not palpable is correct because this is a sign of normal involution, which is the process of the uterus returning to its pre-pregnancy size and shape after delivery. The fundus is the upper part of the uterus that can be felt through the abdomen. Immediately after delivery, the fundus is about the size of a grapefruit and can be felt at or above the umbilicus (the navel). It gradually descends about one fingerbreadth per day until it reaches the level of the symphysis pubis (the joint where the two pubic bones meet) by about 10 days postpartum. By 14 days postpartum, the fundus should be below the symphysis and not palpable.
Choice d) Moderate bright red lochial flow is incorrect because this is not a sign of normal involution, but rather a sign of excessive or prolonged bleeding after delivery. Lochia is the vaginal discharge that consists of blood, mucus, and tissue from the lining of the uterus. It changes in color and amount over time, from red to pink to brown to yellow to white. The normal lochia flow should be scant to moderate in amount, dark red to brown in color, and last for about 4 to 6 weeks postpartum. A moderate bright red lochial flow on day 14 postpartum may indicate that the uterus is not contracting well or that there is an infection or retained placental tissue in the uterus.

Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today