While assessing a client's blood pressure using an aneroid sphygmomanometer, the nurse inflates the cuff to an initial reading of 160 mm Hg. Upon release of the air valve, the nurse immediately hears loud Korotkoff sounds. Which action should the nurse implement next?
Continue the blood pressure assessment until the last Korotkoff sound is heard.
Reposition the stethoscope in the antecubital fossa over the palpable brachial pulse point.
Inflate the cuff quickly to a higher mm Hg reading than the previously auscultated systolic sound.
Release the air and reinflate the cuff to 30 mm Hg above the client's previous systolic reading.
The Correct Answer is D
Choice A reason: Continuing the blood pressure assessment until the last Korotkoff sound is heard is not the best action to implement next. It may result in an inaccurate measurement of the diastolic pressure, as the cuff pressure may be too low to detect the sound.
Choice B reason: Repositioning the stethoscope in the antecubital fossa over the palpable brachial pulse point is not a necessary action to implement next. It may not affect the accuracy of the blood pressure measurement, as the nurse already hears the Korotkoff sounds clearly.
Choice C reason: Inflating the cuff quickly to a higher mm Hg reading than the previously auscultated systolic sound is not a safe action to implement next. It may cause discomfort and injury to the client, as the cuff pressure may be too high and occlude the blood flow.
Choice D reason: Releasing the air and reinflating the cuff to 30 mm Hg above the client's previous systolic reading is the best action to implement next. It helps to avoid the auscultatory gap, which is a period of silence between the systolic and diastolic pressures. It also ensures that the cuff pressure is high enough to detect the true systolic and diastolic pressures.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Choice A reason: This is an incorrect action as it indicates poor posture and balance. The client should walk with the elbows slightly flexed and the shoulders relaxed.
Choice B reason: This is the correct action as it ensures proper fit and comfort of the crutch. The client should fit the crutch 2 finger widths from the axilla to prevent nerve damage and pressure ulcers.
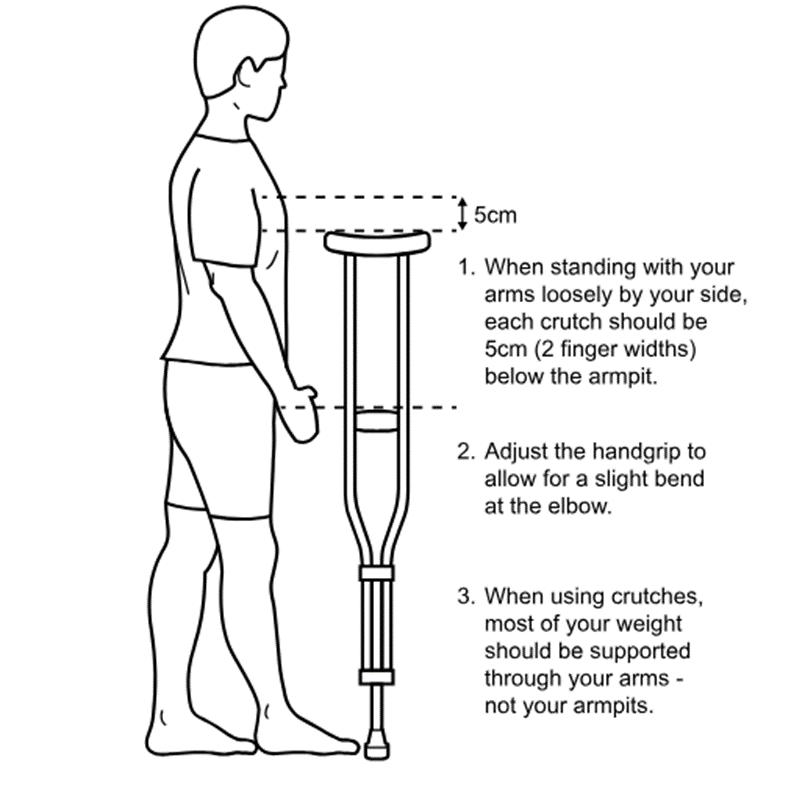
Choice C reason: This is an incorrect action as it may cause pain and injury to the wrists and hands. The client should adjust the height of the hand grips to allow a 30-degree bend at the elbow.
Choice D reason: This is an incorrect action as it may cause instability and falls. The client should hold the crutch 4 to 6 inches (10 to 15 cm) in front and to the side of the foot.
Correct Answer is A
Explanation
Choice A reason:This option is the most therapeutic because it is open-ended and invites the client to express feelings and experiences about the visit. By encouraging the client to talk, the nurse provides an opportunity for the client to explore emotions, which could explain why they became isolative afterward. Open-ended questions also demonstrate interest and support, which fosters trust and promotes communication in therapeutic relationships.
Choice B reason:Asking if the client would like to talk is supportive, but it is too vague and closed-ended. The client may simply answer “yes” or “no,” which does not facilitate deeper exploration of feelings. While it offers availability, it is not as therapeutic as directly encouraging discussion about the observed event, the visit.
Choice C reason: This is a less therapeutic response as it assumes that the client enjoyed the visit. It may not reflect the client's true feelings or experiences. It also limits the client's expression to positive aspects only.
Choice D reason: This is a non-therapeutic response as it labels the client's emotion without validation. It may not accurately describe the client's feeling or situation. It also closes the communication by making a statement instead of asking a question.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today