The nurse observes that a client on a clear liquid diet has a cup of coffee on the breakfast tray. Which action should the nurse implement?
Consult with the dietitian to learn if the client is allowed to drink coffee.
Remind the client that no milk or creamer can be added to the coffee.
Determine which member of the nursing staff brought the cup of coffee to the client.
Remove the coffee from the tray, advising the client that it is not included in the diet.
The Correct Answer is B
Choice A reason: Consulting with the dietitian to learn if the client is allowed to drink coffee is not the best action to take. The nurse should already know the components of a clear liquid diet, which do not include coffee. Coffee is a stimulant that can irritate the gastrointestinal tract and interfere with the healing process.
Choice B reason: This is the correct action. A clear liquid diet allows for transparent liquids that leave no residue, such as black coffee. Adding milk or creamer would render the coffee opaque, making it unsuitable for a clear liquid diet. Therefore, it's appropriate to remind the client to consume the coffee without any additives.
Choice C reason: Determining which member of the nursing staff brought the cup of coffee to the client is not a priority action to take. The nurse should focus on the client's safety and well-being, not on assigning blame or finding fault. The nurse can address the issue with the staff later, after ensuring the client's needs are met.
Choice D reason: Removing the coffee is unnecessary, as black coffee is permitted on a clear liquid diet. Instead, the nurse should ensure the client understands not to add any prohibited substances like milk or creamer.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Choice A reason: This is an incorrect action as it indicates poor posture and balance. The client should walk with the elbows slightly flexed and the shoulders relaxed.
Choice B reason: This is the correct action as it ensures proper fit and comfort of the crutch. The client should fit the crutch 2 finger widths from the axilla to prevent nerve damage and pressure ulcers.
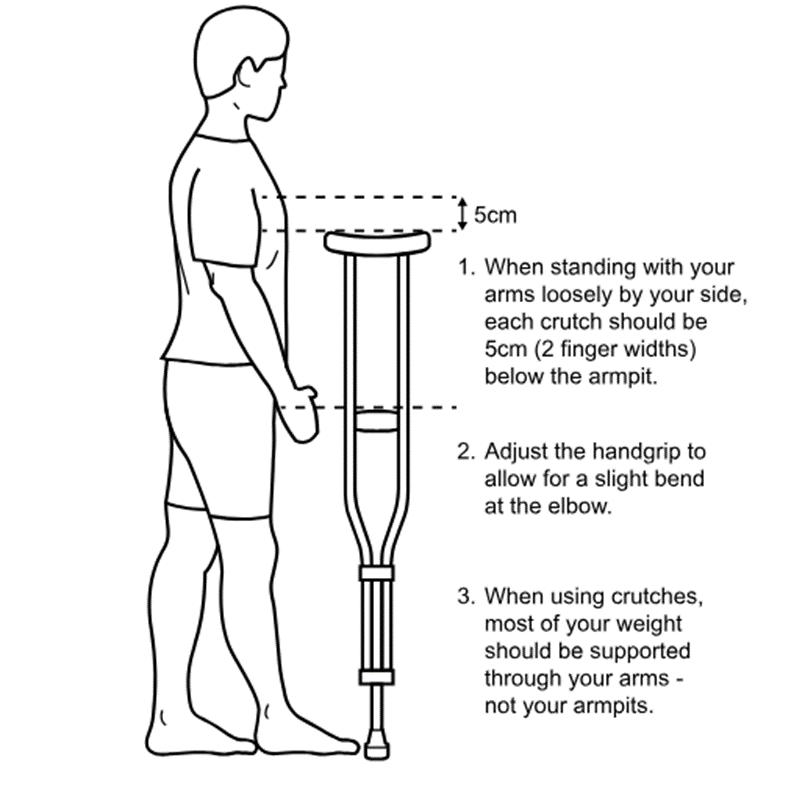
Choice C reason: This is an incorrect action as it may cause pain and injury to the wrists and hands. The client should adjust the height of the hand grips to allow a 30-degree bend at the elbow.
Choice D reason: This is an incorrect action as it may cause instability and falls. The client should hold the crutch 4 to 6 inches (10 to 15 cm) in front and to the side of the foot.
Correct Answer is C
Explanation
Choice A reason: Reviewing the advanced directive document is not the priority action. The nurse should first intervene to clear the airway and prevent aspiration of vomitus.
Choice B reason: Elevating the head of the bed 45 degrees is a good practice, but it is not sufficient to relieve the choking. The nurse should also perform suctioning to remove the vomitus from the mouth and throat.
Choice C reason: Performing oropharyngeal suctioning is the best action as it helps to clear the airway and prevent aspiration of vomitus. The nurse should use a Yankauer suction catheter and apply intermittent suction while moving the catheter around the mouth and throat.
Choice D reason: Irrigating the nasogastric tube with water is not appropriate as it may worsen the vomiting and choking. The nurse should stop the enteral feeding and clamp the tube until the client's condition is stabilized.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today