Which organ is primarily responsible for drug metabolism?
Liver
Lungs
Heart
Kidney
The Correct Answer is A
Choice A reason: This is correct. The liver is the main organ responsible for drug metabolism. The enzymes that the body uses to metabolize drugs are present throughout the body but are most abundant in the liver. The liver can transform drugs into more polar and water-soluble compounds, which can then be excreted by the kidneys or the biliary system.
Choice B reason: This is incorrect. The lungs are not primarily responsible for drug metabolism, although they can play a minor role in some cases. The lungs can metabolize some drugs that are inhaled, such as anesthetics, or drugs that circulate through the pulmonary blood vessels, such as propranolol. However, the lungs have a lower capacity and a lower variety of enzymes than the liver.
Choice C reason: This is incorrect. The heart is not responsible for drug metabolism, although it can be affected by it. The heart is the organ that pumps blood throughout the body, delivering oxygen and nutrients to the tissues and organs. The heart can be influenced by the pharmacokinetics and pharmacodynamics of drugs, which are the processes of drug absorption, distribution, metabolism, and excretion, and the effects of drugs on the body, respectively.
Choice D reason: This is incorrect. The kidney is not primarily responsible for drug metabolism, although it is important for drug excretion. The kidney is the organ that filters the blood and removes waste products and excess fluid as urine. The kidney can excrete drugs that are water-soluble or that are not reabsorbed by the tubules. The kidney can also metabolize some drugs, such as aspirin, but to a lesser extent than the liver.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
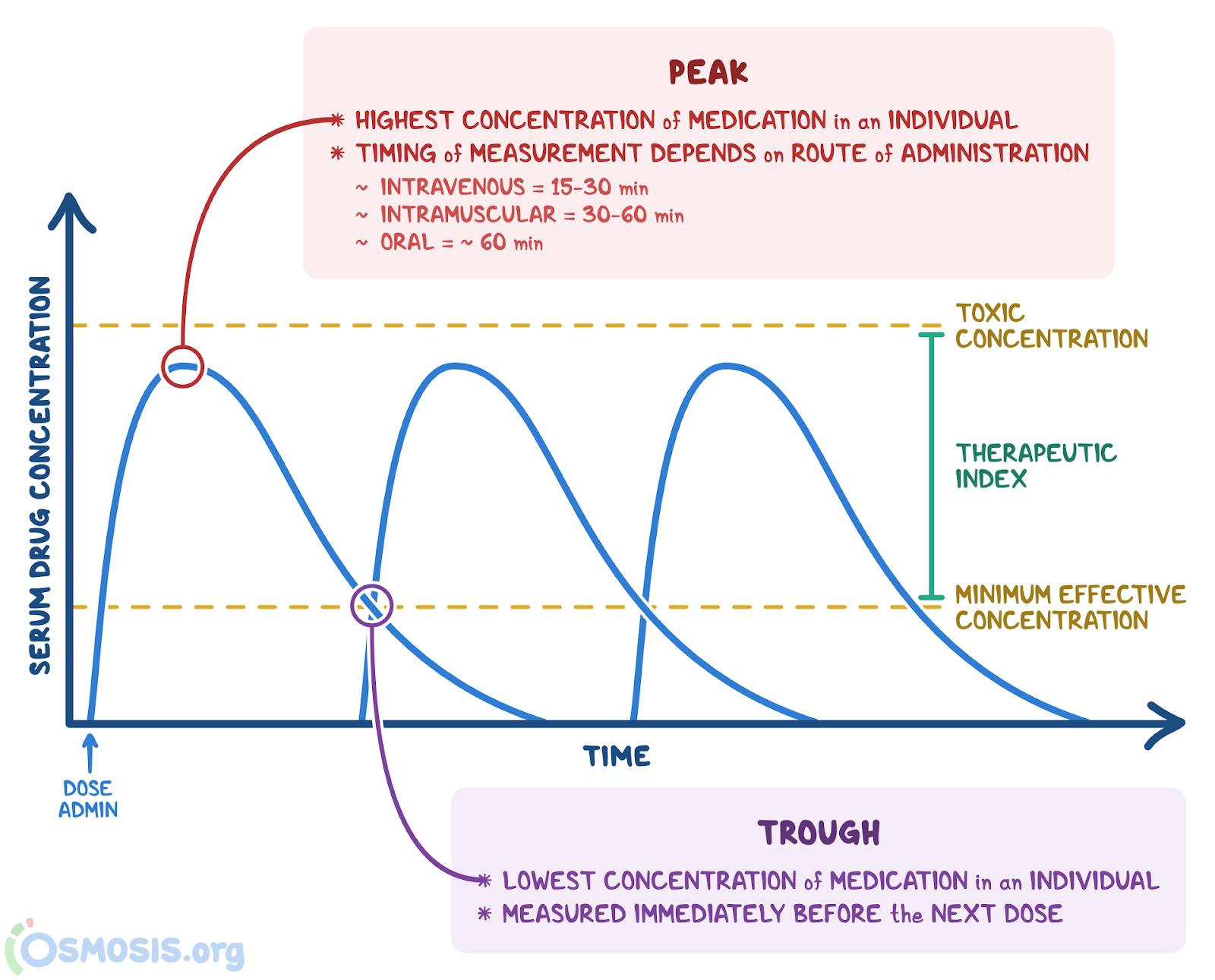
Choice A reason: Peak level is the correct term to describe the highest concentration of a drug in the blood after it is administered. Peak level is also known as peak plasma concentration or Cmax, and it reflects the rate and extent of drug absorption. Peak level is influenced by factors such as the route of administration, the dose, the formulation, and the bioavailability of the drug. Peak level is important to monitor for drugs that have a narrow therapeutic range, meaning that there is a small difference between the effective and toxic doses. The nurse should measure the peak level at the appropriate time after the drug administration, and adjust the dose or the frequency as needed to achieve the desired therapeutic effect and avoid adverse effects .
Choice B reason: Halflife is not the correct term to describe the highest concentration of a drug in the blood after it is administered. Halflife is the time it takes for the concentration of a drug in the blood to decrease by 50%. Halflife reflects the rate of drug elimination, which depends on factors such as the metabolism and excretion of the drug. Halflife is important to determine the dosing interval and the time to reach steady state. The nurse should consider the halflife of the drug when prescribing or administering the drug, and avoid drug accumulation or subtherapeutic levels .
Choice C reason: Trough level is not the correct term to describe the highest concentration of a drug in the blood after it is administered. Trough level is the lowest concentration of a drug in the blood before the next dose is given. Trough level reflects the balance between drug absorption and elimination, and it indicates the minimum effective concentration of the drug. Trough level is important to monitor for drugs that have a narrow therapeutic range, meaning that there is a small difference between the effective and toxic doses. The nurse should measure the trough level just before the next dose of the drug, and adjust the dose or the frequency as needed to achieve the desired therapeutic effect and avoid adverse effects .
Choice D reason: Steady state is not the correct term to describe the highest concentration of a drug in the blood after it is administered. Steady state is the condition when the rate of drug administration is equal to the rate of drug elimination, and the concentration of the drug in the blood remains constant. Steady state is usually reached after four to five halflives of the drug, and it reflects the optimal therapeutic level of the drug. Steady state is important to maintain for drugs that have a long halflife or a narrow therapeutic range, meaning that there is a small difference between the effective and toxic doses. The nurse should ensure that the drug is administered at regular intervals and at the appropriate dose to achieve and maintain steady state.
Correct Answer is C
Explanation
Choice A reason: This is incorrect. SQ (subcutaneous) administration involves injecting a drug into the fatty tissue under the skin. This route is slower than IV or IM administration, as the drug has to diffuse through the tissue before reaching the bloodstream.
Choice B reason: This is incorrect. PO (by mouth) administration involves swallowing a drug and absorbing it through the digestive system. This route is the slowest of all, as the drug has to pass through the stomach and the liver before reaching the bloodstream. The drug may also be affected by the first pass effect, which reduces its bioavailability.
Choice C reason: This is correct. IV (intravenous) administration involves injecting a drug directly into a vein. This route is the fastest of all, as the drug enters the bloodstream immediately and reaches the target site quickly. The drug also has 100% bioavailability, meaning none of it is lost or degraded.
Choice D reason: This is incorrect. IM (intramuscular) administration involves injecting a drug into a muscle. This route is faster than SQ or PO administration, as the drug can be absorbed by the capillaries in the muscle. However, it is still slower than IV administration, as the drug has to cross the muscle membrane before reaching the bloodstream.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today