The PN Identifies that the client is having a tonic-clonic seizure. The oxygen saturation is 40% and the respiratory rate is 4 breaths/min. The PN calls for help and 2 other PNs enter the room. Which three actions will the PN anticipate taking next?
Begin chest compressions.
Watch the seizure activity and document the time and client movement.
Place pillows around the bed rails to provide padding.
Stop the IV fluids.
Increase the supplemental oxygen to 10 L/min via nasal cannula.
Manually ventilate the client with a bag-valve mask.
Correct Answer : C,E,F
C. Place pillows around the bed rails to provide padding: During a tonic-clonic seizure, the client may experience uncontrolled movements and convulsions. Placing pillows around the bed rails helps prevent injury by providing padding and cushioning.
E. Increase the supplemental oxygen to 10 L/min via nasal cannula: The client's oxygen saturation is dangerously low at 40%. Increasing the supplemental oxygen to 10 L/min via nasal cannula will help improve oxygenation and prevent hypoxia.
F. Manually ventilate the client with a bag-valve-mask: Since the respiratory rate is only 4 breaths/min, the client is not adequately ventilating on their own. Manual ventilation with a bag-valve mask will provide necessary oxygenation and ventilation support during the seizure.
The other options are not appropriate actions at this time:
- Begin chest compressions: Chest compressions are indicated if the client's heart has stopped or if they are in cardiac arrest. Since the scenario describes a seizure, the client's heart is presumed to be functioning.
- Watch the seizure activity and document the time and client movement: Although documentation is important, during an active seizure, the priority is to ensure the client's safety and provide immediate interventions. Documentation can be done after the seizure has ended.
- Stop the IV fluids: There is no indication to stop the IV fluids based on the given information. IV fluids are generally continued unless there is a specific reason to discontinue them.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is ["A","D"]
Explanation
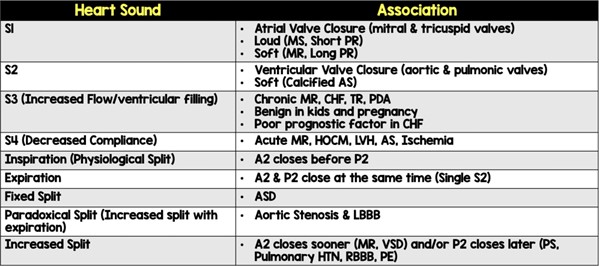
S3 is an extra heart sound that occurs during diastole (the filling phase of the cardiac cycle). It is commonly associated with conditions such as heart failure and volume overload. S3 is often described as a low-frequency, dull, and distant sound heard after S2 (the second heart sound).
B, C- S1, and S2 are the normal heart sounds that are typically heard in all individuals. S1 is the first heart sound, heard as "lub," and is caused by the closure of the mitral and tricuspid valves. S2 is the second heart sound, heard as "dub," and is caused by the closure of the aortic and pulmonic valves. These sounds are normal and expected.
S4 is another abnormal heart sound, which occurs during late diastole and is associated with conditions such as ventricular hypertrophy and reduced ventricular compliance.
Correct Answer is B
Explanation
This is the first action the PN should take when noticing that the UAP consistently records subnormal temperatures when using a tympanic thermometer. Observing how the UAP obtains temperatures will help the PN identify any errors or problems with the technique, equipment, or documentation. The PN can then provide feedback and guidance to the UAP to ensure accurate and reliable temperature measurements.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today