The nurse is using the PED model to write a nursing diagnosis. Which nursing diagnoses demonstrate that the nurse used this model appropriately? Select all that apply.
Ineffective Breathing Pattern as evidenced by cyanotic lips.
Risk for infection related to recent surgery.
Nutrition less than adequate related to anxiety as evidenced by weight loss of ten pounds.
Ineffective coping related to depression as evidenced by a suicide attempt.
Noncompliance (DASH diet) related to denial of having the disease.
Correct Answer : A,C,D
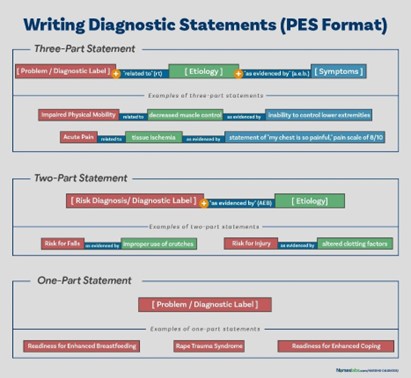
The PED model is a framework for writing nursing diagnoses that stands for Problem, Etiology, and Defining Characteristics. A nursing diagnosis written using the PED model includes a statement of the client's problem (P), the cause or contributing factors of the problem (E), and the observable signs and symptoms that indicate the presence of the problem (D). In this case, options a), c), and d) are examples of nursing diagnoses that demonstrate appropriate use of the PED model. Each of these diagnoses includes a statement of the client's problem, the cause or contributing factors, and the defining characteristics that indicate the presence of the problem.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
It would be inappropriate to delegate the unsupervised task of transferring a client from bed to chair to an unlicensed assistant (UAP) if it was the client's first time out of bed after surgery. In this situation, the client may have specific needs or limitations that require the expertise and assessment of a licensed healthcare provider. The nurse should supervise the transfer to ensure that it is performed safely and appropriately for the client's condition.
Correct Answer is A
Explanation
In this situation, the nurse is performing the role of an educator. The nurse is explaining the procedures for preventing infection in a central venous access device to the spouse and demonstrating how to hook the client to the medication infusion.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today