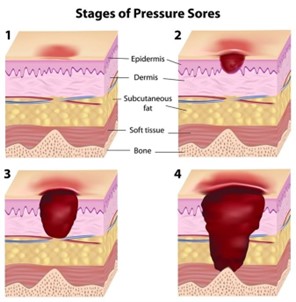
While performing a bed bath, the nurse notes an area of tissue injury on the client's sacral area. The wound presents as a shallow open ulcer with a red-pink wound bed and partial thickness loss of dermis. What is the correct name of this wound?
Stage II pressure ulcer
Stage IV pressure ulcer
Stage I pressure ulcer
Stage III pressure ulcer
The Correct Answer is A
A stage II pressure ulcer is a wound that presents as a shallow open ulcer with a red-pink wound bed and partial thickness loss of dermis. This type of wound is caused by unrelieved pressure on the skin, resulting in damage to the underlying tissue. In this scenario, the nurse notes an area of tissue injury on the client's sacral area that matches the description of a stage II pressure ulcer. Stage I pressure ulcers are characterized by non-blanchable erythema of intact skin, while stage III and IV pressure ulcers involve full-thickness tissue loss and may expose underlying muscle, bone, or other structures.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
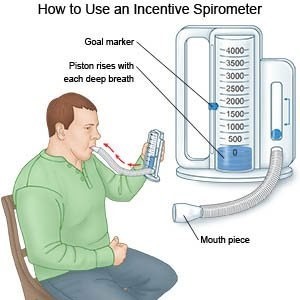
When providing education to a postoperative client on how to use an incentive spirometer, an accurate step that should be included in the education plan is to instruct the client to inhale slowly and as deeply as possible through the mouthpiece without using the nose ¹⁴. This helps the client to take deep breaths and fully expand their lungs. The other options (Instruct the client to inhale normally and then place the lips securely around the mouthpiece, Encourage the client to perform incentive spirometry 2 to 3 times every 1 to 2 hours, if possible, and When the client cannot inhale anymore, the client should hold his breath and count to 10) are not accurate steps that should be included in the education plan.
Correct Answer is C
Explanation
The Agent-Host-Environment Model is a model of health promotion and illness prevention that focuses on the interaction between an infectious agent, the host (the person who is infected), and the environment in which the infection occurs. In this case, the agent is Clostridium difficile, the host is the elderly resident, and the environment is the long-term care facility where the outbreak occurred. The prescription of metronidazole (Flagyl) by the resident's primary care provider is an example of an intervention ai

Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today