The nurse is caring for a group of clients with the help of a practical nurse (PN). Which nursing action(s) should the nurse assign to the PN? (Select all that apply)
Obtain postoperative vital signs for a client one day following unilateral knee arthroplasty.
Perform daily surgical dressing change for a client who had an abdominal hysterectomy.
Initiate patient controlled analgesia (PCA. pumps for two clients immediately postoperatively.
Start the second blood transfusion for a client twelve hours following a below knee amputation.
Monitor a dose of warfarin per protocol for a client with type 2 diabetes mellitus (DM).
Correct Answer : A,B,E
Choice C reason: Initiating patient controlled analgesia (PCA. pumps for two clients immediately postoperatively is not a nursing action that can be assigned to the PN. PCA pump is a device that allows the client to self-administer pain medication through an IV line by pressing a button. PCA pump should be initiated by the nurse after verifying the prescription, setting the parameters, educating the client, and ensuring safety and effectiveness. The PN does not have the authority or competency to initiate PCA pump or adjust its settings.
Choice D reason: Starting the second blood transfusion for a client twelve hours following a below knee amputation is not a nursing action that can be assigned to the PN. Blood transfusion is a procedure that delivers donated blood or blood products into the client's bloodstream through an IV line. Blood transfusion should be started by the nurse after verifying the prescription, checking the blood type and compatibility, obtaining informed consent, and monitoring for any adverse reactions. The PN does not have the authority or competency to start blood transfusion or manage its complications.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
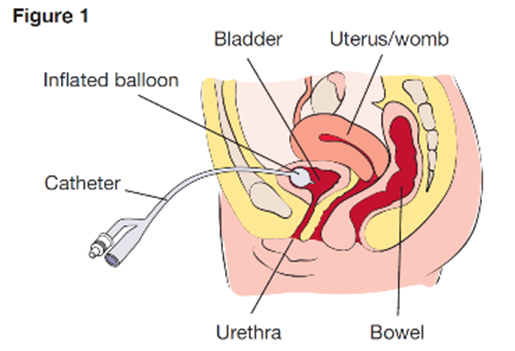
Choice A: Observing the insertion site of the suprapubic catheter is an essential assessment for the home health nurse, as this can help detect any signs of infection, inflammation, or leakage. Therefore, this is the correct choice.
Choice B: Palpating the flank area is not a necessary assessment for the home health nurse, as this is not related to the suprapubic catheter. This is a distractor choice.
Choice C: Measuring abdominal girth is not a relevant assessment for the home health nurse, as this is not affected by the suprapubic catheter. This is another distractor choice.
Choice D: Assessing the perineal area is not an important assessment for the home health nurse, as this is not involved in the suprapubic catheter. This is another distractor choice.
Correct Answer is B
Explanation
Choice A reason: A 16-year-old client diagnosed with major depression who refuses to participate in group does not require the nurse's immediate attention. Depression is a mood disorder that causes persistent feelings of sadness, hopelessness, and loss of interest. Refusing to participate in group may indicate low motivation, social withdrawal, or poor self-esteem, which are common symptoms of depression. The nurse should respect the client's preference and offer alternative activities or individual therapy.
Choice B reason:This client requires immediate intervention because pacing can be a sign of agitation, restlessness, or escalating mania. Clients with bipolar disorder in a manic phase may exhibit increased energy, impulsivity, irritability, and even aggression. If not addressed promptly, this behavior could escalate to disruptive outbursts, impulsive actions, or even violence toward themselves or others. The nurse should intervene by using calm communication, redirection, and possibly medication if prescribed to help de-escalate the situation and ensure safety.
Choice Creason:This scenario involves peer conflict, which is important to address, but it does not necessarily indicate an immediate risk of harm. Clients with antisocial behavior often engage in conflict due to manipulative or confrontational tendencies, but being yelled at does not mean they are in immediate danger. The nurse should monitor the situation and intervene to prevent escalation, but other safety concerns take priority.
Choice D reason: A 14-year-old client with anorexia nervosa who is refusing to eat the evening snack does not require the nurse's immediate attention. Anorexia nervosa is an eating disorder that causes extreme restriction of food intake and fear of weight gain. Refusing to eat the evening snack may indicate distorted body image, dietary rules, or anxiety, which are common factors of anorexia nervosa. The nurse should encourage the client to eat and provide support and education.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today