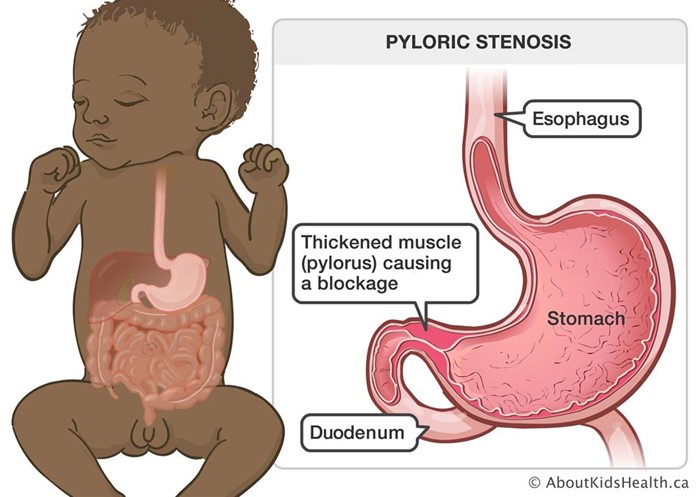
A 6-week-old infant with pyloric stenosis is scheduled for a pyloromyotomy. Which pre-operative nursing action has the highest priority?
Mark an outline of the "olive-shaped" mass in the right epigastric area.
Instruct parents regarding care of the incisional area.
Monitor amount of intake and infant's response to feedings.
Initiate a continuous infusion of IV fluids per prescription.
The Correct Answer is D
Choice A reason: Marking an outline of the "olive-shaped" mass in the right epigastric area is not a priority nursing action. The mass is caused by hypertrophy of the pyloric sphincter, which obstructs gastric emptying and causes projectile vomiting. The mass may not be palpable in all cases.
Choice B reason: Instructing parents regarding care of the incisional area is a post-operative nursing action, not a pre-operative one. The parents will need to learn how to keep the incision clean and dry, monitor for signs of infection, and administer pain medication as prescribed.
Choice C reason: Monitoring amount of intake and infant's response to feedings is important, but not the highest priority. The infant may have difficulty feeding due to nausea, vomiting, and abdominal pain.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Choice A: Providing bedside equipment for transmission and protective precautions is not the first action that the nurse should implement, as this is a standard precaution that should be already in place for all clients in the critical care unit. This is a distractor choice.
Choice B: Evaluating daily serum electrolytes and hydration status is not the first action that the nurse should implement, as this is a routine assessment that can be done later after addressing the immediate problem of infection. This is another distractor choice.
Choice C: Culturing sputum, urine, burn wound, and all intravenous access sites is the first action that the nurse should implement, as this can help identify the source and type of infection, which can guide the appropriate antibiotic therapy and prevent further complications. Therefore, this is the correct choice.
Choice D: Implementing central line-associated bloodstream infection (CLABSI) protocols is not the first action that the nurse should implement, as this is a preventive measure that may not be applicable for this client who already has SIRS. This is another distractor choice.
Correct Answer is ["B","C","E","F"]
Explanation
Choice B is correct because weight management is an important factor in preventing and controlling hypertension. Taking daily walks for thirty minutes can help reduce weight and lower blood pressure.
Choice C is correct because salt substitutes can help with maintaining a healthy diet by reducing sodium intake. Sodium intake is associated with increased blood pressure and should be limited to less than 2,300 mg per day.
Choice E is correct because sodium intake can be regulated by rinsing canned foods in water. Canned foods often contain high amounts of sodium as a preservative and rinsing them can remove some of the excess sodium.
Choice F is correct because uncontrolled hypertension can lead to renal damage. Hypertension can cause damage to the blood vessels and impair the function of the kidneys, leading to chronic kidney disease or failure.
Choice A is incorrect because alcohol consumption can produce vascular changes that increase blood pressure. Alcohol intake should be limited to no more than one drink per day for women and two drinks per day for men.
Choice D is incorrect because blood pressure readings should not be taken at noontime. Blood pressure readings should be taken at the same time each day, preferably in the morning before breakfast or in the evening before dinner.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today