The nurse is caring for a client diagnosed with schizophrenia. Which of the following should the nurse identify as findings consistent with schizophrenia? (Select all that apply.)
Schizophrenia can be cured with antidepressants.
Schizophrenia typically first presents in adolescence or early adulthood.
Antipsychotic medications can be used to manage symptoms of hallucinations and delusions.
Some clients with schizophrenia have a higher risk of substance abuse disorders.
Schizophrenia affects thoughts and perceptions.
Correct Answer : B,C,D,E
Choice A Reason:
Schizophrenia cannot be cured with antidepressants. Antidepressants may be used to treat comorbid depression in individuals with schizophrenia, but they do not address the core symptoms of schizophrenia itself. Schizophrenia is a chronic condition that typically requires lifelong treatment with antipsychotic medications to manage symptoms.
Choice B Reason:
Schizophrenia typically first presents in adolescence or early adulthood. This is the period when symptoms such as hallucinations, delusions, and disorganized thinking often first become apparent. The onset of schizophrenia during this developmental stage can significantly impact an individual's social and vocational abilities.
Choice C Reason:
Antipsychotic medications are the cornerstone of schizophrenia treatment. They can be used to manage symptoms of hallucinations and delusions, which are known as positive symptoms of schizophrenia. These medications work by affecting neurotransmitters in the brain, particularly dopamine.
Choice D Reason:
Individuals with schizophrenia have a higher risk of substance abuse disorders. Substance use can exacerbate symptoms of schizophrenia and complicate the course of the illness. It is important for treatment plans to address any co-occurring substance use disorders.
Choice E Reason:
Schizophrenia significantly affects thoughts and perceptions. It can cause distorted thinking patterns, false beliefs, and sensory experiences that others do not share. These symptoms can be distressing and may lead to difficulties in distinguishing reality.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is ["A","D"]
Explanation
Choice A Reason:
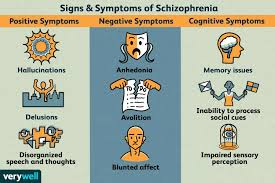
Blunted affect refers to a significant reduction in the intensity of emotional expression. In the context of schizophrenia, a person with blunted affect may show less facial expression, have diminished expressive gestures, and a monotone voice. This symptom reflects a decrease in the expression of emotions, which is characteristic of the negative symptoms of schizophrenia.
Choice B Reason:
Delusions are a type of positive symptom of schizophrenia, not a negative one. They are false beliefs that are not based in reality, such as thinking one has superpowers or is being persecuted. Delusions represent an excess or distortion of normal functions.
Choice C Reason:
Poor judgment is not typically classified as a negative symptom of schizophrenia. It can be a consequence of cognitive impairments or positive symptoms like delusions but is not a negative symptom itself.
Choice D Reason:
Anhedonia is the inability to feel pleasure and is a core negative symptom of schizophrenia. Individuals with anhedonia may not enjoy activities that they used to find pleasurable, which can significantly impact their quality of life.
Choice E Reason:
Hallucinations, like delusions, are considered positive symptoms of schizophrenia. They involve experiencing sensations that are not present, such as hearing voices or seeing things that others do not see.
Correct Answer is D
Explanation
Choice A Reason:
Passive-aggressive communication involves expressing negative feelings indirectly rather than openly addressing them. It often manifests as sarcasm, backhanded compliments, or subtle digs. In this scenario, the client is directly stating their preference without any indirect negativity, so it is not passive-aggressive.
Choice B Reason:
Aggressive communication is characterized by speaking in a way that violates or disrespects others. It often includes yelling, interrupting, or demeaning language. The client's statement does not display any of these characteristics; instead, it is a straightforward expression of their wish.
Choice C Reason:
Nonassertive communication, also known as passive communication, occurs when individuals fail to express their thoughts or feelings, or they do so without confidence. The client in the garden is clearly stating their desire to plant the sunflower, which is not indicative of a nonassertive pattern.
Choice D Reason:
Assertive communication is the act of expressing one's opinions, feelings, and needs in a clear, direct, and respectful way. It involves standing up for oneself while also considering the rights and feelings of others. The client's statement, "I would really like to plant the sunflower," is a clear, direct expression of their preference, making it an assertive form of communication.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today