The nurse is auscultating heart sounds on a client and hears an extra sound late in diastole, just before the S1. How should the nurse document this finding?
The third heart sound (S3)
A friction rub
The fourth heart sound (S4)
A split second heart sound S2
The Correct Answer is A
A. The third heart sound (S3):
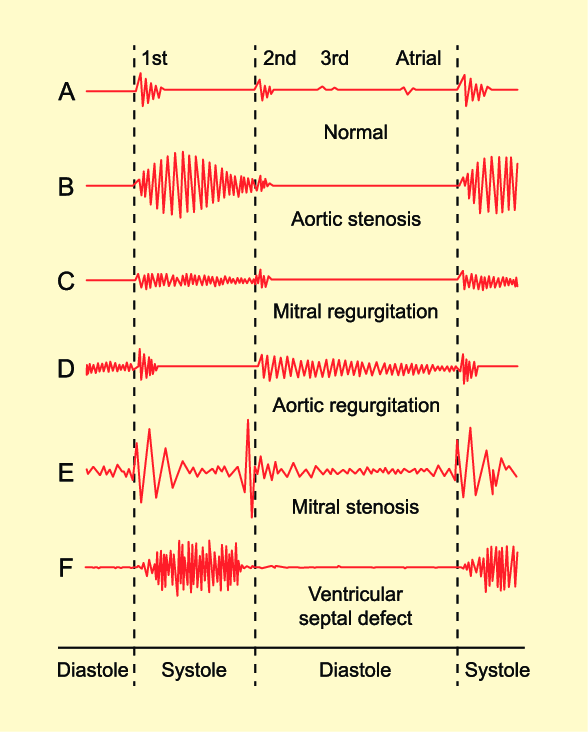
The third heart sound (S3) is an abnormal heart sound that occurs during early diastole, immediately after S2 (the second heart sound). It is caused by the rapid filling of the ventricles and is often associated with conditions like heart failure. In heart failure, the ventricles become stiff, causing vibrations that produce the S3 sound.
B. A friction rub:
A friction rub is a high-pitched, scratchy sound heard during both systole and diastole. It is caused by the rubbing together of inflamed pericardial layers (pericarditis) and is usually heard best at the left lower sternal border. Friction rubs can indicate pericardial inflammation and are often heard in conditions such as pericarditis or after a myocardial infarction.
C. The fourth heart sound (S4):
The fourth heart sound (S4) occurs late in diastole, just before S1, and is caused by atrial contraction. It is associated with increased resistance to ventricular filling, often due to conditions like hypertension or aortic stenosis. The S4 sound is heard as a low-pitched "atrial gallop."
D. A split second heart sound S2:
The second heart sound (S2) represents the closure of the aortic and pulmonic valves. Normally, S2 has two components: A2 (aortic valve closure) and P2 (pulmonic valve closure). A split S2 occurs when A2 and P2 do not close simultaneously. A physiological split S2 is common during inspiration and occurs due to delayed closure of the pulmonic valve. An abnormal or fixed split S2 can indicate underlying heart conditions such as atrial septal defect (ASD) or right bundle branch block (RBBB).
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
A. AV node - SA node - bundle of His - bundle branches:
This sequence is incorrect. The SA node (sinoatrial node) initiates the electrical impulse in the heart, followed by the AV node (atrioventricular node), bundle of His, and then the bundle branches.
B. SA node - AV node - bundle of His - bundle branches:
This sequence is correct. The electrical stimulus of the cardiac cycle starts at the SA node, which is the natural pacemaker of the heart. From the SA node, the impulse travels to the AV node, then to the bundle of His, and finally to the bundle branches, which distribute the impulse to the ventricles, causing them to contract.
C. Bundle of His - AV node - SA node - Erb's Point:
This sequence is incorrect. Erb's Point is a point on the chest where heart sounds S2 and S3 can be heard most distinctly.
D. AV node - SA node - bundle of His - Erb's Point:
This sequence is incorrect. The AV node comes after the SA node in the electrical conduction system of the heart. Erb's Point is not a part of the normal cardiac conduction pathway; it is a location for auscultation on the chest.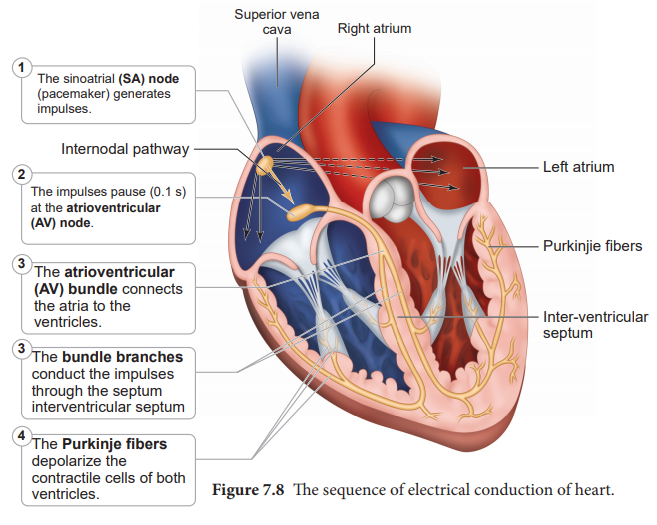
Correct Answer is A
Explanation
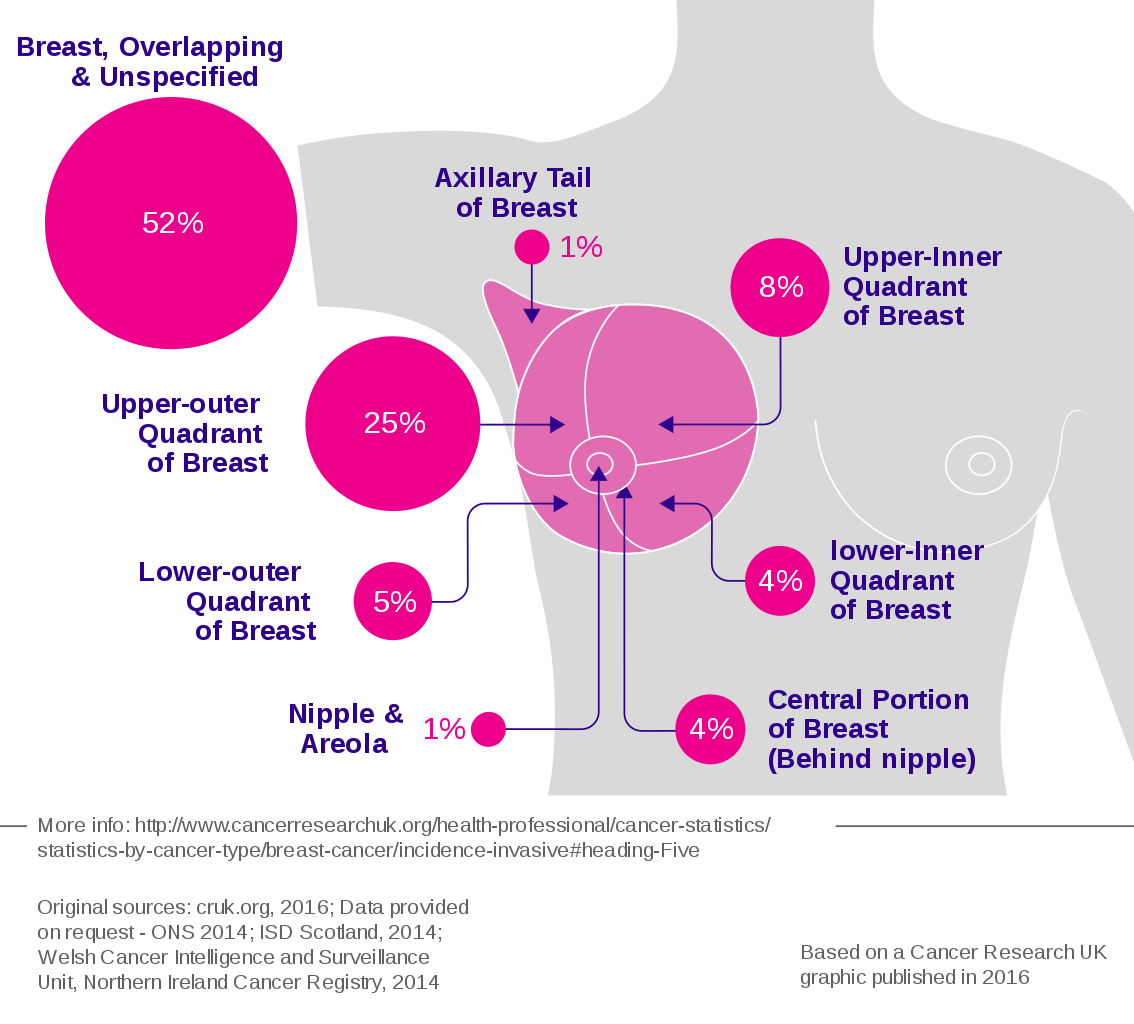
A. The location of most breast tumors: This choice is correct. The upper outer quadrant of the breast is the most common site for breast tumors. This area has a higher concentration of glandular tissue, making it more susceptible to the development of tumors. Therefore, thorough examination of this area is crucial during breast examinations.
B. More prone to Injury and calcifications than other locations in the breast: While injuries can occur in any part of the breast, the statement about calcifications is not accurate. Calcifications in breast tissue can occur in various areas and are not specific to the upper outer quadrant.
C. The largest quadrant of the breast: This statement is not accurate. The breast quadrants are not distinguished by size; they are anatomical divisions used for reference during breast examinations. Each quadrant has its significance for examination purposes, but none is considered the largest.
D. Where most of the suspensory ligaments attach: The suspensory ligaments, also known as Cooper's ligaments, provide structural support to the breast tissue. While they are essential for breast anatomy, they are not concentrated in the upper outer quadrant exclusively. These ligaments are distributed throughout the breast tissue.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today