The nurse is testing a client's visual accommodation. Which of the following should the nurse recognize as an assessment finding from visual accommodation?
The pupils constrict when the examiner's index finger slowly moves toward the client's nose.
The client involuntary blinks in the presence of bright light directed over the pupils during the eye exam.
The client's peripheral vision becomes sharper when the examiner shines a light over the pupils.
The pupils dilate when the examiner's index finger slowly moves toward the client's nose.
The Correct Answer is A
A. The pupils constrict when the examiner's index finger slowly moves toward the client's nose.
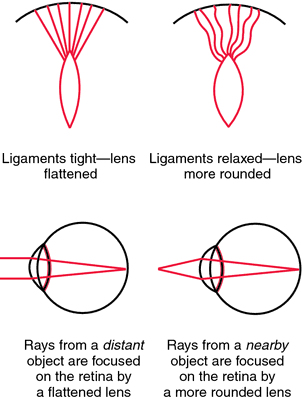
This statement is correct. Visual accommodation is the process by which the eye's lens changes shape to focus on objects at varying distances. When an object moves closer to the eyes, the pupils constrict to adjust and focus on the near object, preventing double vision.
B. The client involuntarily blinks in the presence of bright light directed over the pupils during the eye exam.
This statement describes the pupillary light reflex, not visual accommodation. The pupillary light reflex is the response of the pupils to light exposure.
C. The client's peripheral vision becomes sharper when the examiner shines a light over the pupils.
This statement is not accurate. Peripheral vision sharpness is not related to visual accommodation. Visual accommodation mainly involves adjusting focus for objects at varying distances.
D. The pupils dilate when the examiner's index finger slowly moves toward the client's nose.
This statement is incorrect. Pupils should constrict, not dilate, when focusing on a near object (as in visual accommodation). Dilation occurs in low-light conditions or in response to sympathetic stimulation.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
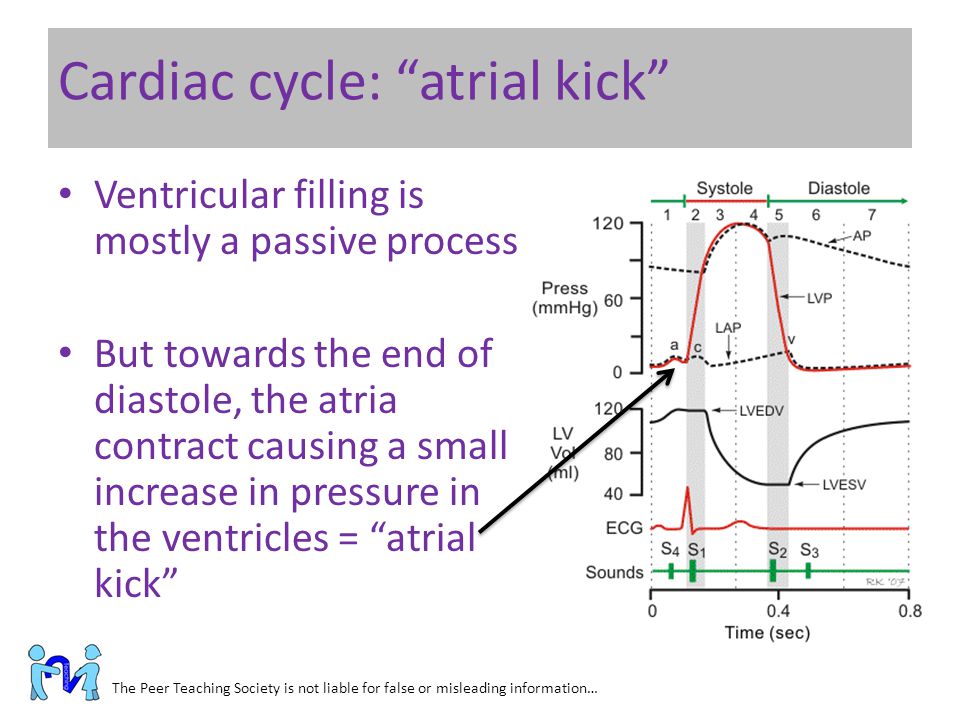
A. The atria contract toward the end of diastole and push the remaining blood into the ventricles.
This choice is correct. During atrial systole (atrial contraction), the atria contract, pushing the remaining blood into the ventricles. This additional filling of the ventricles optimizes cardiac output.
B. The atria contract during systole and attempt to push against closed valves.
This statement is incorrect. The atria do not contract during systole; they contract during diastole (atrial systole) to fill the ventricles.
C. Atrial kick is the pressure exerted against the atria as the ventricles contract during systole.
This statement is incorrect. Atrial kick refers to the atrial contraction, not the pressure exerted against the atria.
D. Contraction of the atria at the beginning of diastole can be felt as a palpitation.
This statement is not entirely accurate. A palpitation is a sensation of rapid or strong heartbeat, which might be felt during various cardiac events, not specifically during atrial contraction at the beginning of diastole.
Correct Answer is D
Explanation
. Presence of breath sounds: While assessing the anterior chest, the nurse should listen for breath sounds over various areas of the lungs. However, this is related to auscultation, not inspection.
B. Diaphragmatic excursion: Diaphragmatic excursion involves assessing the movement of the diaphragm during breathing. This is typically done by percussing the level where dullness changes to resonance during inhalation and exhalation. It is more related to percussion, not inspection.
C. Symmetric chest expansion: Symmetric chest expansion refers to the equal expansion of both sides of the chest during inhalation. The nurse can observe and palpate the chest to assess if it expands symmetrically on both sides. This is a crucial aspect of the inspection of the anterior chest.
D. Shape and configuration of the chest wall: The shape and configuration of the chest wall, including abnormalities or deformities, should be assessed during inspection. This includes observing for any asymmetry, deformities, masses, or scars on the anterior chest.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today