The nurse is auscultating the lungs of a sleeping client and hears short, popping, crackling breath sounds that stop after a few breaths. The nurse recognizes that these breath sounds are:
Atelectatic crackles that do not have a pathologic cause.
Vesicular breath sounds.
Fine wheezes.
Fine crackles and may be a sign of pneumonia.
The Correct Answer is A
A. Atelectatic crackles that do not have a pathologic cause:
Atelectatic crackles are short, popping, crackling sounds heard during auscultation. They occur in individuals who are in a supine position and disappear after a few breaths. These crackles are not indicative of any pathological condition; they are common when the lungs are not fully aerated, especially when a person is lying down.
B. Vesicular breath sounds:
Vesicular breath sounds are normal lung sounds heard over the peripheral lung areas. They are soft, low-pitched, and continuous throughout inspiration and part of expiration. Vesicular breath sounds are the typical sounds heard during routine breathing and are not associated with crackling or popping noises.
C. Fine wheezes:
Wheezes are high-pitched whistling sounds heard during expiration. They occur due to narrowed airways and are commonly associated with conditions like asthma or bronchoconstriction. Fine wheezes suggest a partial obstruction in the smaller airways, causing turbulent airflow, leading to the characteristic sound.
D. Fine crackles and may be a sign of pneumonia:
Fine crackles are high-pitched, discontinuous, crackling sounds heard during inspiration. They can occur due to the sudden opening of small airways, and their presence may indicate fluid in the lungs or lung inflammation. Fine crackles are often associated with conditions such as pneumonia, heart failure, or interstitial lung diseases.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
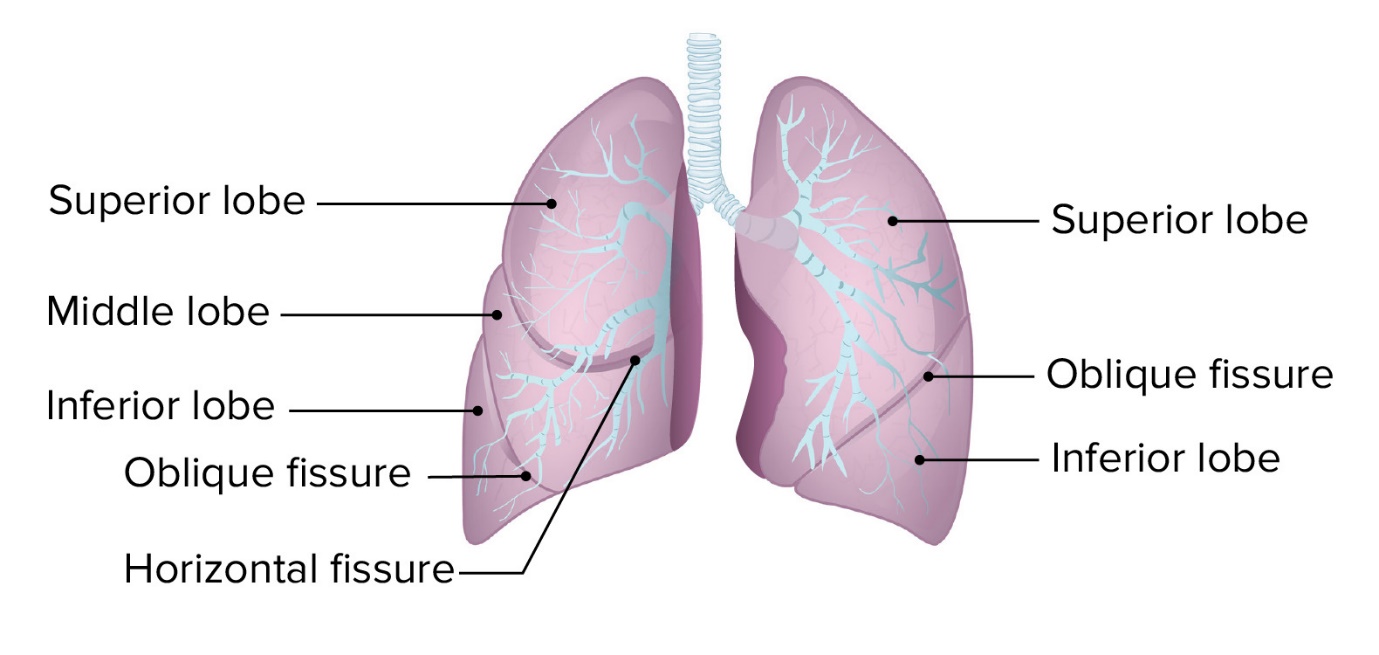
A. Consists of two lobes.
This statement is correct. The left lung consists of two lobes: the upper lobe and the lower lobe. The right lung, not the left lung, has three lobes: upper, middle, and lower lobes.
B. Primarily consists of an upper lobe on the posterior chest.
This statement is not accurate. The upper lobe of the left lung is present in the anterior and posterior parts of the chest. It is not limited to the posterior chest.
C. Is shorter than the right lung because of the underlying stomach.
This statement is not correct. The left lung is not shorter due to the underlying stomach. The left lung is slightly smaller than the right lung to accommodate the space for the heart, but this size difference is not due to the stomach.
D. Is divided by the horizontal fissure.
This statement is not accurate. The left lung is not divided by the horizontal fissure. The horizontal fissure is a feature of the right lung, not the left lung. The left lung is divided by the oblique fissure into the upper and lower lobes
Correct Answer is D
Explanation
A. Indicates the beginning of diastole: This statement is not accurate. S2, the second heart sound, indicates the end of systole and the beginning of diastole. It is specifically associated with the closure of the aortic and pulmonary valves.
B. Coincides with the carotid artery pulse: This statement is not accurate. S2 is associated with the closure of the aortic and pulmonary valves in the heart, not with the carotid artery pulse.
C. Is louder than an S1: This statement is not accurate. S1, the first heart sound, is usually louder than S2. S1 is associated with the closure of the mitral and tricuspid valves and marks the beginning of systole.
D. Is caused by the closure of the semilunar valves: This statement is accurate. S2 is caused by the closure of the aortic and pulmonary valves, which are the semilunar valves in the heart. It marks the end of systole and the beginning of diastole.

Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today