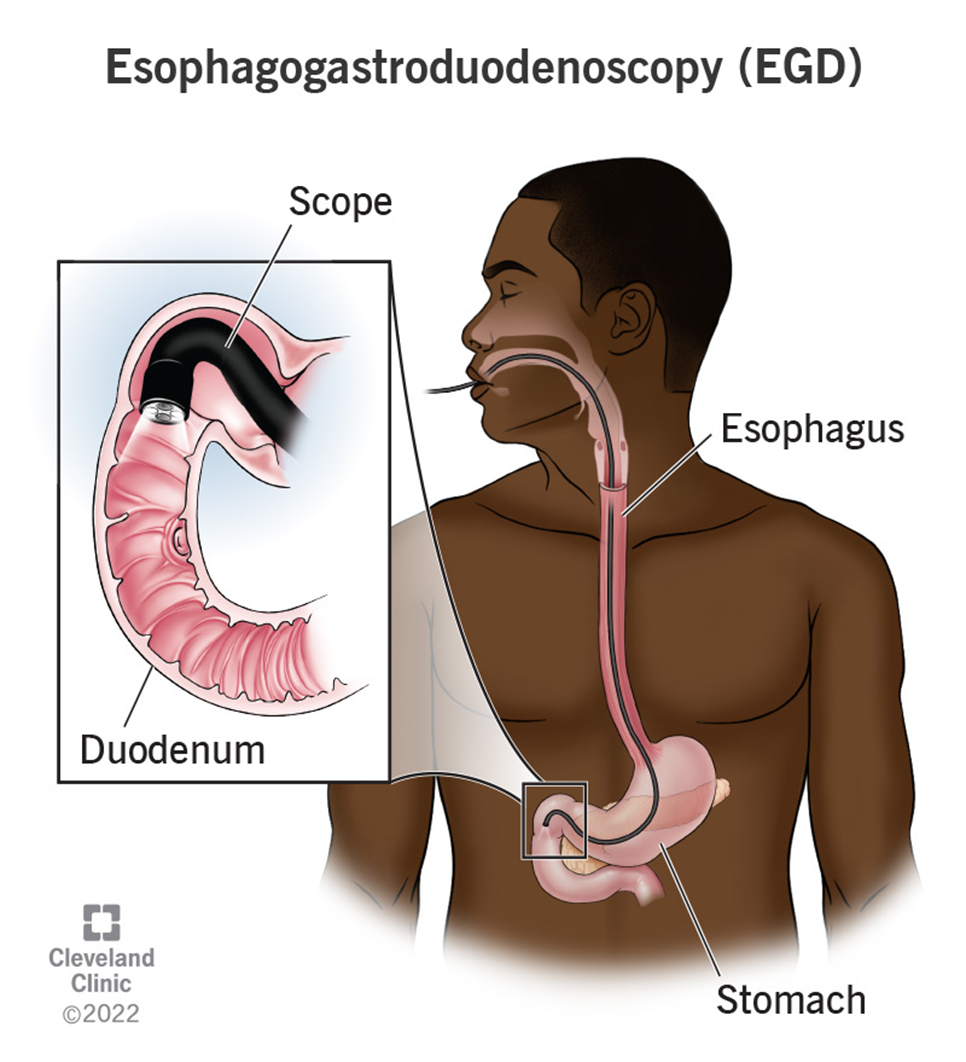
The nurse is caring for a client recovering from an esophagogastroduodenoscopy (EGD). Which of the following client symptoms would require further nursing assessment?
Thirst
Sore throat
Abdominal distention
Drowsiness
The Correct Answer is C
Choice A Reason:
Thirst is a common and expected symptom after an EGD, especially if the client has been fasting before the procedure. It does not typically indicate a complication and can be managed by gradually reintroducing fluids as tolerated. Therefore, thirst does not require further nursing assessment beyond routine post-procedure care.
Choice B Reason:
A sore throat is also a common symptom following an EGD. The procedure involves passing an endoscope through the throat, which can cause temporary irritation and discomfort. This symptom usually resolves on its own within a few days and does not indicate a serious complication. Therefore, a sore throat does not require further nursing assessment beyond providing comfort measures such as lozenges or warm saltwater gargles.
Choice C Reason:
Abdominal distention is a concerning symptom that requires further nursing assessment. It can indicate complications such as perforation, bleeding, or infection following the EGD. Perforation of the gastrointestinal tract is a rare but serious complication that can lead to peritonitis and sepsis if not promptly addressed. Therefore, any signs of abdominal distention should be reported to the provider immediately for further evaluation and intervention.
Choice D Reason:
Drowsiness is a common side effect of the sedatives used during the EGD procedure. It is expected that the client may feel drowsy or sleepy for a few hours after the procedure as the sedative wears off. This symptom does not typically require further nursing assessment unless it persists for an unusually long time or is accompanied by other concerning symptoms such as difficulty breathing or altered mental status.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is ["B","C"]
Explanation
Choice A Reason: High-flow nasal cannula
The high-flow nasal cannula (HFNC) is designed to deliver oxygen at flow rates much higher than 5 liters per minute, typically ranging from 20 to 60 liters per minute. It is used for patients requiring high levels of oxygen and positive airway pressure. Therefore, it is not appropriate for a flow rate of 5 liters per minute.
Choice B Reason: Simple face mask
The simple face mask is suitable for delivering oxygen at flow rates between 6 to 10 liters per minute. However, it can also be used at a flow rate of 5 liters per minute, providing an FiO2 (fraction of inspired oxygen) of approximately 40-60%. This makes it an appropriate choice for the given requirement.
Choice C Reason: Nasal cannula
The nasal cannula is a low-flow oxygen delivery device that can deliver oxygen at flow rates from 1 to 6 liters per minute. At 5 liters per minute, it provides an FiO2 of approximately 40%. It is comfortable for patients and is commonly used for those who need a moderate amount of supplemental oxygen.
Choice D Reason: Non-rebreather mask
The non-rebreather mask is designed to deliver high concentrations of oxygen, typically at flow rates of 10 to 15 liters per minute. It is used in situations where patients need a high FiO2, close to 100%. Therefore, it is not suitable for a flow rate of 5 liters per minute.
Choice E Reason: Venturi mask
The Venturi mask is used to deliver precise oxygen concentrations, typically ranging from 24% to 60% FiO2. It is suitable for patients who require controlled oxygen therapy. While it can be adjusted to deliver oxygen at a flow rate of 5 liters per minute, it is generally used for more specific FiO2 requirements.
Correct Answer is ["A","C","D","E"]
Explanation
Choice A: Instruct the patient to withhold any medication for diuretic therapy.
Reason: Diuretics can lead to dehydration and electrolyte imbalances, which can complicate the cardiac catheterization procedure. Withholding diuretics helps to maintain fluid balance and reduce the risk of complications during the procedure
Choice B: Prepare to administer fluids 2 hours before the procedure for patients with renal dysfunction.
Reason: Administering fluids before the procedure helps to prevent contrast-induced nephropathy, especially in patients with renal dysfunction. Hydration helps to flush out the contrast material used during the procedure, reducing the risk of kidney damage.
Choice C: Advise the patient to take all anticoagulants.
Reason: This choice is incorrect. Patients are usually advised to withhold anticoagulants before a cardiac catheterization to reduce the risk of bleeding complications. The decision to continue or withhold anticoagulants should be based on a careful assessment of the patient’s risk of thromboembolism versus the risk of bleeding.
Choice D: Administer steroids if the patient has an allergy to iodine-based contrast.
Reason: Administering steroids is a common premedication strategy for patients with a known allergy to iodine-based contrast media. Steroids help to reduce the risk of an allergic reaction during the procedure.
Choice E: Ensure that the patient is NPO for a minimum of 2 hours before the procedure.
Reason: Ensuring that the patient is NPO (nothing by mouth) helps to reduce the risk of aspiration during the procedure. Typically, patients are advised to be NPO for 6-8 hours before the procedure, but a minimum of 2 hours is essential.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today