Before administering an antibiotic that can cause nephrotoxicity, which laboratory value is most important for the practical nurse (PN) to review?
Serum calcium
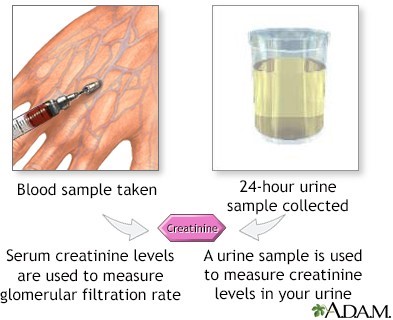
Serum creatinine
Hemoglobin and Hematocrit
White blood cell count (WBC)
The Correct Answer is B
Serum creatinine is the most important laboratory value to review before administering an antibiotic that can cause nephrotoxicity. Nephrotoxicity is an alteration in the function of the kidney due to exposure to certain drugs or toxins.
It can be assessed by measuring the glomerular filtration rate (GFR), which is the rate of clearance of a substance from the blood by the kidneys. Serum creatinine is a waste product of muscle metabolism that is freely filtered by the glomeruli and not reabsorbed or secreted by the tubules.
Therefore, it is a reliable indicator of GFR and renal function. An increase in serum creatinine indicates a decrease in GFR and renal function, which may be caused by nephrotoxic drugs.
The other laboratory values are not directly related to nephrotoxicity or GFR:
- Serum calcium: This may be affected by renal function, but it is not a sensitive or specific marker of nephrotoxicity. It may be altered by other factors such as vitamin D, parathyroid hormone, and bone metabolism.
- Hemoglobin and hematocrit: These may be affected by renal function, but they are not sensitive or specific markers of nephrotoxicity. They may reflect the erythropoietin production by the kidneys, which stimulates red blood cell production in the bone marrow. However, they may also be influenced by other factors such as blood loss, hydration status, and iron deficiency.
- White blood cell count (WBC): This is not related to nephrotoxicity or GFR. It may reflect the presence of infection or inflammation, which may be a cause or a consequence of renal impairment, but it is not a direct measure of renal function.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is ["1"]
Explanation
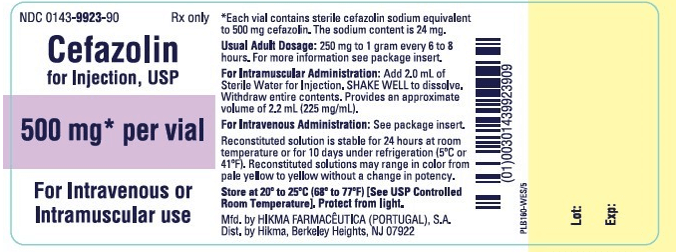
This is the correct answer because the concentration of cefazolin after reconstitution is 1 gram/2.5 mL, which is equivalent to 400 mg/1 mL. Therefore, to administer 400 mg of cefazolin, the PN should draw up 1 mL of the reconstituted solution. This can be calculated using the formula:
Desired dose / Available dose = Volume to administer
400 mg / 1000 mg = x mL / 2.5 mL
x = (400 x 2.5) / 1000
x = 1 mL
Correct Answer is A
Explanation
Choice A rationale:
Impaired physical mobility relative to muscle rigidity has the highest priority in the nursing care plan for a client diagnosed with Parkinson's disease. Parkinson's disease is characterized by motor symptoms such as muscle rigidity, bradykinesia, and postural instability. Impaired physical mobility can significantly impact a patient's ability to perform activities of daily living and maintain independence. Addressing this issue is crucial to enhance the patient's quality of life and prevent complications such as falls.
Choice B rationale:
While the risk for aspiration relative to muscle weakness is a valid concern in Parkinson's disease, impaired physical mobility takes precedence as it directly affects the patient's ability to move, ambulate, and perform daily activities. Addressing mobility issues is fundamental to maintaining overall functioning and independence.
Choice C rationale:
The risk for constipation relative to immobility is important to address, but it is not the highest priority. Impaired physical mobility can lead to multiple complications, including constipation. However, improving mobility should be the primary focus to prevent a wide range of issues associated with Parkinson's disease.
Choice D rationale:
Self-care deficit relative to motor disturbance is a concern in Parkinson's disease, but it is not the highest priority. Impaired physical mobility directly impacts a patient's ability to engage in self-care activities. By addressing mobility issues first, the nurse can facilitate the patient's ability to perform self-care tasks more independently in the long run.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today