An emergency department client is diagnosed with a hip dislocation. The client's family is relieved that the client has not suffered a hip fracture, but the nurse explains that this is still considered to be a medical emergency. What is the rationale for the nurse's statement?
The longer the joint is displaced, the more difficult it is to get it back in place.
Avascular necrosis may develop at the site if it is not promptly resolved.
The client's pain will increase until the joint is realigned.
Dislocation can become permanent if the process of bone remodeling begins.
The Correct Answer is A
A. The longer the joint is displaced, the more difficult it is to get it back in place:
This statement is correct. Prompt reduction of a dislocated joint is important because the longer the joint remains out of place, the more difficult it becomes to realign it. Delayed reduction can lead to complications and makes the process more challenging for healthcare providers.
B. Avascular necrosis may develop at the site if it is not promptly resolved:
Avascular necrosis is a condition where bone tissue dies due to a lack of blood supply. While it is a potential complication of hip dislocation, it is not the immediate rationale for considering hip dislocation a medical emergency. The urgency primarily lies in the difficulty of reducing the dislocation and preventing further complications.
C. The client's pain will increase until the joint is realigned:
This statement is partially correct. While it is true that dislocated joints are extremely painful, the urgency in reducing the dislocation is not solely based on pain management. It is essential to prevent complications, restore joint function, and minimize long-term damage to the affected area.
D. Dislocation can become permanent if the process of bone remodeling begins:
This statement is accurate. If a dislocated joint is not promptly reduced, the surrounding tissues may undergo changes, and the process of bone remodeling can begin. This can lead to the dislocation becoming more difficult or even impossible to reduce, resulting in a permanent dislocation. Early intervention is essential to prevent this outcome.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
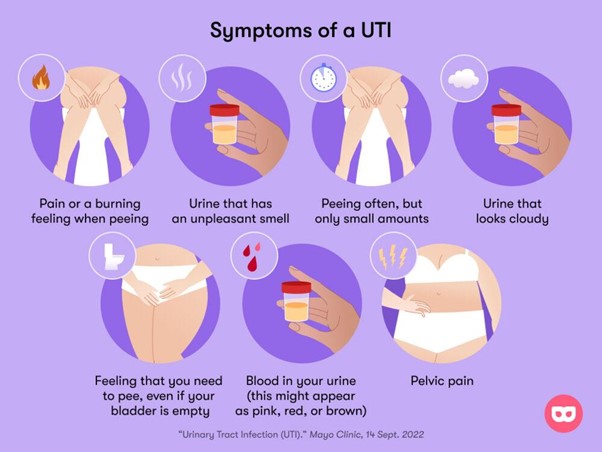
A. Urinary tract infection
The symptoms described, including recent mental status changes and periods of incontinence, are suggestive of a urinary tract infection (UTI) in an elderly individual. UTIs are common among older adults and can cause a variety of symptoms, including confusion, which is often the primary manifestation in the elderly population. Other symptoms can include urinary urgency, frequency, and incontinence.
B. Acute kidney failure - While acute kidney failure can cause changes in urination and mental status, it is less likely to be the primary cause of these symptoms in this scenario. UTI is a more common and immediate concern given the symptoms described.
C. Septic shock - Septic shock is a severe condition that occurs when an infection leads to a life-threatening drop in blood pressure. While septic shock can cause altered mental status, it is a critical condition that often presents with more dramatic symptoms and requires immediate intensive care management. The symptoms described are more suggestive of a UTI.
D. Urinary stasis - Urinary stasis refers to the slowing or cessation of urine flow. While urinary stasis can contribute to the development of UTIs, it is not a condition that would cause sudden and acute mental status changes and incontinence on its own. UTI is a more likely cause of the symptoms described.
Correct Answer is A
Explanation
A. Inadequate immobilization: Proper immobilization is essential for fractured bones to heal correctly. Immobilization, often achieved through casts, splints, or other orthopedic devices, stabilizes the broken bone fragments, allowing them to fuse back together. If the immobilization is not sufficient or if the patient doesn't follow the prescribed immobilization protocol, there can be excessive movement at the fracture site, hindering the healing process.
B. Venous thromboembolism: Venous thromboembolism (VTE) refers to the formation of blood clots in veins, usually in the legs (deep vein thrombosis) that can travel to the lungs (pulmonary embolism). While VTE is a potential complication after a fracture, it is not a direct cause of delayed bone union.
C. Inadequate vitamin D intake: Vitamin D is essential for bone health as it helps the body absorb calcium, which is crucial for bone formation and maintenance. Inadequate vitamin D levels can weaken bones and impair the healing process, but it's not a common cause of delayed bone union unless there are severe deficiencies or underlying medical conditions.
D. Bleeding at the injury site: Bleeding at the injury site occurs immediately after the fracture and is a natural part of the body's response to injury. While excessive bleeding can lead to complications, it is not a likely cause of delayed bone union six weeks after the injury. In the early stages of healing, bleeding is replaced by the formation of a hematoma, which eventually transforms into a callus and aids in the bone healing process.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today