A female client has been experiencing recurrent urinary tract infections. What health education should the nurse provide to this client?
Void every 6 to 8 hours.
Avoid voiding immediately after sexual intercourse.
Take a bubble bath daily and keep the perineal region clean.
Increase the daily amount of water consumed.
The Correct Answer is D
A. Void every 6 to 8 hours:This interval may not be frequent enough. It is generally recommended to void every 2 to 3 hours to help flush out bacteria and reduce the risk of infection.
B. Avoid voiding immediately after sexual intercourse.This is not recommended. It is actually advised to void immediately after sexual intercourse to help flush out any bacteria that may have entered the urethra.
C. Take a bubble bath daily and keep the perineal region clean:
While keeping the perineal region clean is important for general hygiene, taking bubble baths and using heavily scented products can irritate the urethra and potentially increase the risk of UTIs. The nurse should advise against frequent bubble baths and suggest using mild, unscented soaps for the perineal area.
D. Increase the daily amount of water consumed:
Drinking more water helps increase urine output, which helps flush out bacteria from the urinary tract and can reduce the risk of recurrent UTIs.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
A. Morse Scale:
The Morse Scale, also known as the Morse Fall Scale, is used to assess a patient's risk of falling. It evaluates various factors such as history of falling, secondary diagnosis, ambulatory aids, IV therapy, gait, and mental status. It is primarily focused on assessing the risk of falls, not pressure ulcers.
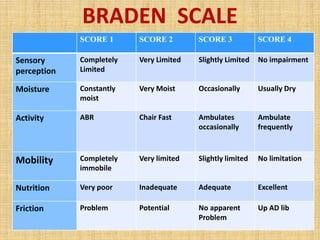
B. Braden Scale:
As previously mentioned, the Braden Scale assesses a patient's risk for developing pressure ulcers. It takes into account sensory perception, moisture, activity, mobility, nutrition, and friction/shear. The scale helps healthcare providers determine the level of risk a patient has for developing pressure sores and guides interventions to prevent them.
C. Bristol Scale:
The Bristol Stool Scale is used to classify the form of human feces into seven categories. It is a medical aid designed to classify the form of human feces into seven categories. This scale is primarily used to assess bowel movements and is unrelated to pressure ulcers.
D. Hendrich II Scale:
The Hendrich II Fall Risk Model is a tool designed to identify patients at risk for falls. It includes factors such as confusion, symptomatic depression, altered elimination, dizziness, male gender, and the use of antiepileptics, benzodiazepines, or non-opioid analgesics. Similar to the Morse Scale, it focuses on assessing the risk of falls, not pressure ulcers.
Correct Answer is A
Explanation
A. Urine culture and sensitivity
Explanation: A urine culture and sensitivity test involves growing bacteria from a urine sample in a laboratory setting. Once the bacteria have grown, they are exposed to different antibiotics to see which one is most effective in inhibiting their growth. This helps healthcare providers identify the specific strain of bacteria causing the infection and choose the most appropriate antibiotic treatment.
B. Serum creatinine level
Explanation: Serum creatinine level is a blood test used to measure kidney function. It evaluates how well the kidneys are filtering waste from the blood. While important for assessing kidney health, it does not determine the specific bacteria causing a urinary tract infection or the appropriate antibiotic treatment.
C. Urinalysis
Explanation: Urinalysis is a broad screening test that assesses various components in the urine, such as red and white blood cells, protein, glucose, and bacteria. While it can detect signs of a urinary tract infection (such as the presence of bacteria and white blood cells), it does not identify the specific bacterial strain causing the infection or provide information about antibiotic sensitivity.
D. Kidney scan
Explanation: A kidney scan, also known as a renal scan, is a medical imaging technique used to assess the structure and function of the kidneys. It can help diagnose conditions like kidney stones, urinary obstruction, or kidney infections. However, it does not determine the strain of bacteria causing a urinary tract infection or guide antibiotic treatment.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today