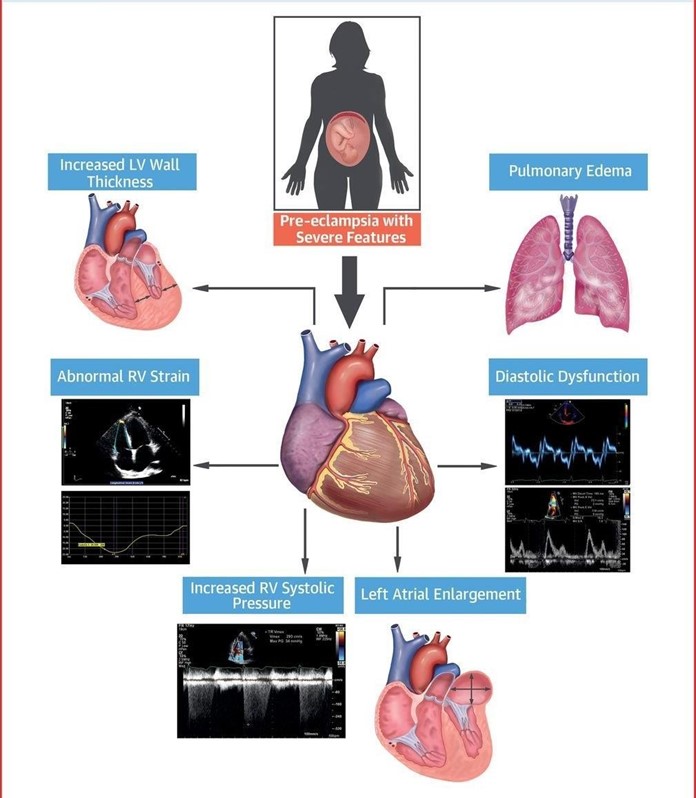
A woman with severe preeclampsia is being treated with bed rest and intravenous magnesium sulfate. The drug classification of this medication is
Antihypertensive
Anticonvulsant
Tocolytic
Diuretic
The Correct Answer is B
Choice A) Antihypertensive: This is not the correct classification of magnesium sulfate. Antihypertensives are drugs that lower blood pressure, such as beta blockers, calcium channel blockers, or angiotensin-converting enzyme inhibitors. Magnesium sulfate does not have a significant effect on blood pressure, and it is not used as a primary treatment for hypertension in preeclampsia.
Choice B) Anticonvulsant: This is the correct classification of magnesium sulfate. Anticonvulsants are drugs that prevent or reduce the frequency and severity of seizures, such as phenytoin, valproic acid, or carbamazepine.
Magnesium sulfate is used as a prophylactic and therapeutic agent for eclampsia, which is a life-threatening complication of preeclampsia characterized by seizures. Magnesium sulfate acts by blocking the neuromuscular transmission and reducing the cerebral edema and vasospasm.
Choice C) Tocolytic: This is not the correct classification of magnesium sulfate. Tocolytics are drugs that inhibit uterine contractions and delay preterm labor, such as terbutaline, nifedipine, or indomethacin. Magnesium sulfate is not effective as a tocolytic agent, and it is not recommended for this purpose by the American College of Obstetricians and Gynecologists.
Choice D) Diuretic: This is not the correct classification of magnesium sulfate. Diuretics are drugs that increase urine output and reduce fluid retention, such as furosemide, hydrochlorothiazide, or spironolactone. Magnesium sulfate does not have a diuretic effect, and it can cause fluid overload and pulmonary edema if administered in excess.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
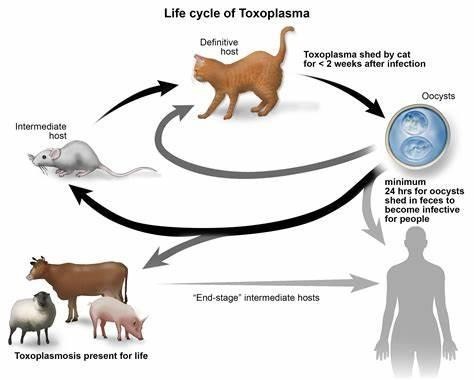
Choice a) I will be certain to empty the litter boxes regularly is incorrect because this is a risky behavior for a pregnant woman who wants to prevent toxoplasmosis. Toxoplasmosis is an infection caused by a parasite called Toxoplasma gondii, which can be found in the feces of cats and other animals. If a pregnant woman gets infected with toxoplasmosis, she can pass it to her unborn baby, which can cause serious problems such as miscarriage, stillbirth, or birth defects. Therefore, a pregnant woman should avoid contact with cat litter and let someone else handle the litter boxes, or wear gloves and wash her hands thoroughly if she has to do it herself.
Choice b) I have to wash all of my fruits and vegetables is correct because this is a good practice for a pregnant woman who wants to prevent toxoplasmosis. Toxoplasmosis can also be transmitted through contaminated soil or water, which can adhere to fruits and vegetables. Therefore, a pregnant woman should wash all of her fruits and vegetables before eating them, and peel or cook them if possible, to remove any traces of the parasite.
Choice c) I won't eat raw eggs is correct because this is another good practice for a pregnant woman who wants to prevent toxoplasmosis. Toxoplasmosis can also be acquired through eating undercooked or raw meat or eggs that contain the parasite. Therefore, a pregnant woman should avoid eating raw eggs or any foods that contain them, such as mayonnaise, mousse, or homemade ice cream, and cook all of her meat and eggs thoroughly until they are no longer pink or runny.
Choice d) I need to be cautious when cooking meat is correct because this is also an important practice for a pregnant woman who wants to prevent toxoplasmosis. Toxoplasmosis can also be spread through handling raw meat that contains the parasite. Therefore, a pregnant woman should be careful when cooking meat and use separate utensils and cutting boards for raw and cooked meat, wash her hands and surfaces after touching raw meat, and avoid tasting raw meat while cooking it.
Correct Answer is D
Explanation
Choice a) Urine output of 200 mL for the past 8 hours is incorrect because this is a normal finding for a postpartum woman. The average urine output for a healthy adult is about 800 to 2000 mL per day, which means about 100 to 250 mL per hour. Therefore, a urine output of 200 mL for the past 8 hours is within the normal range and does not indicate any complications.
Choice b) Weight decrease of 2 pounds since delivery is incorrect because this is also a normal finding for a postpartum woman. The weight loss is due to the expulsion of the placenta, amniotic fluid, and blood during delivery. A postpartum woman can expect to lose about 10 to 12 pounds immediately after giving birth, and another 5 pounds in the following weeks due to fluid loss. Therefore, a weight decrease of 2 pounds since delivery is not a cause for concern and does not need to be reported to the obstetrician.
Choice c) Pulse rate of 65 beats per minute is incorrect because this is also a normal finding for a postpartum woman. The normal resting pulse rate for an adult ranges from 60 to 100 beats per minute, and it may decrease slightly after delivery due to blood loss and reduced cardiac output. Therefore, a pulse rate of 65 beats per minute is not indicative of any problems and does not require any intervention.
Choice d) Drop in hematocrit of 6% since admission is correct because this is an abnormal finding for a postpartum woman and suggests that she has developed anemia due to excessive blood loss. Hematocrit is the percentage of red blood cells in the blood, and it reflects the oxygen-carrying capacity of the blood. The normal hematocrit range for an adult female is 37% to 47%, and it may decrease slightly after delivery due to hemodilution. However, a drop in hematocrit of more than 10% from the baseline or below 30% indicates severe anemia and requires immediate treatment. Therefore, a drop in hematocrit of 6% since admission is a significant change that should be reported to the obstetrician as soon as possible.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today