A nurse on an antepartum unit is receiving change-of-shift report for four clients. Which of the following clients should the nurse assess first?
A client who is at 12 weeks of gestation and is experiencing nausea and vomiting
A client who is at 34 weeks of gestation and is experiencing epigastric pain and headache
A client who is at 38 weeks of gestation and is experiencing painful urination
A client who is at 39 weeks of gestation and is experiencing cramping and spotting
The Correct Answer is B
Among the given options, the client who is at 34 weeks of gestation and experiencing epigastric pain and headache should be assessed first. Epigastric pain and headache can be signs of preeclampsia, a serious condition characterized by high blood pressure and organ dysfunction during pregnancy. Preeclampsia requires immediate attention as it can lead to complications for both the mother and the fetus.
Option a) A client at 12 weeks of gestation experiencing nausea and vomiting may be experiencing normal symptoms of early pregnancy. While it is important to assess the client's well-being, it is not an immediate priority compared to the potential signs of preeclampsia in option b.
Option c) A client at 38 weeks of gestation experiencing painful urination may indicate a urinary tract infection (UTI). While a UTI should be addressed, it does not pose the same level of immediate risk as the potential signs of preeclampsia in option b.
Option d) A client at 39 weeks of gestation experiencing cramping and spotting may be in early labor or have other signs of impending labor. While it is important to assess this client's condition, it is not an immediate priority compared to the potential signs of preeclampsia in option b.
Therefore, the nurse should assess the client who is at 34 weeks of gestation and experiencing epigastric pain and headache as the first priority. Prompt evaluation and management of preeclampsia symptoms are crucial to prevent complications and ensure the well-being of both the mother and the fetus.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
Sore nipples are a common problem for breastfeeding mothers, especially in the first few days or weeks after delivery. They can cause pain, discomfort, and frustration, and may interfere with breastfeeding success and satisfaction. The most common cause of sore nipples is poor latch, which means that the newborn does not attach to the breast correctly and does not suckle effectively. Poor latch can result from various factors, such as improper positioning, tongue-tie, inverted or flat nipples, engorgement, or thrush.
The nurse should assess the newborn's latch while breastfeeding to identify and correct any problems that may cause sore nipples. The nurse should observe the following signs of a good latch:
- The newborn's mouth is wide open and covers most of the areola (the dark area around the nipple).
- The newborn's chin and nose touch the breast, and the cheeks are rounded and not dimpled.
- The newborn's tongue is visible under the lower lip and curls around the breast.
- The newborn's lips are flanged outwards and not tucked inwards.
- The newborn's jaw moves rhythmically and smoothly, and swallowing sounds are audible.
- The mother feels a gentle tugging sensation on the nipple, but no pain or pinching.
The nurse should also teach the mother how to achieve a good latch by using different positions, supporting the breast with her hand, tickling the newborn's lower lip with her nipple, and bringing the newborn to the breast when their mouth is wide open. The nurse should also encourage the mother to seek help from a lactation consultant or a peer support group if she has persistent or severe nipple pain.
a) Instructing the client to wait 4 hours between daytime feedings is not an appropriate action for the nurse to take. This may reduce nipple soreness temporarily, but it can also cause breast engorgement, milk supply reduction, mastitis, or poor weight gain in the newborn. The nurse should advise the client to feed the newborn on demand, usually every 1.5 to 3 hours during the day and every 3 to 4 hours at night.
b) Offering supplemental formula between the newborn's feedings is not an appropriate action for the nurse to take. This may interfere with breastfeeding initiation and establishment, as it can reduce the mother's milk supply, confuse the newborn's sucking pattern, increase the risk of nipple preference or rejection, and expose the newborn to potential allergens or infections. The nurse should support exclusive breastfeeding for the first six months of life, unless there is a medical indication for supplementation.
c) Having the client limit the length of breastfeeding to 5 minutes per breast is not an appropriate action for the nurse to take. This may not be enough time for the newborn to get enough milk, especially the hindmilk that is richer in fat and calories. It may also prevent proper drainage of the breast and lead to engorgement or mastitis. The nurse should advise the client to let the newborn feed until they are satisfied and release the breast on their own, which may take 10 to 20 minutes per breast on average.

Correct Answer is D
Explanation
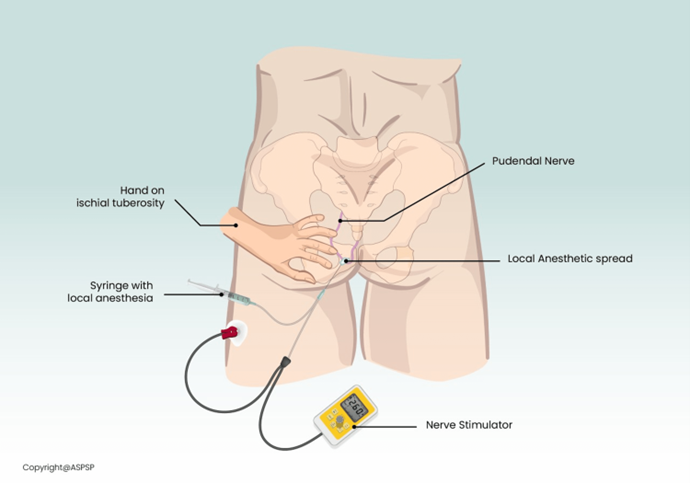
A pudendal nerve block is a local anesthetic administered to block the pudendal nerve, which supplies sensation to the perineum and external genitalia. It is commonly used during childbirth to provide pain relief during the second stage of labor.
An adverse effect of a pudendal nerve block is a decreased ability to bear down, or a decreased ability to push effectively during labor. This is because the block affects the nerves responsible for the contraction of the pelvic floor muscles, which are necessary for effective pushing during delivery.
Option a) Uterine hyperstimulation is not an adverse effect of a pudendal nerve block. Uterine hyperstimulation refers to excessive contractions of the uterus, often caused by medications such as oxytocin. Pudendal nerve block does not directly affect uterine contractions.
Option b) Maternal hypertension is not an adverse effect of a pudendal nerve block. Hypertension refers to
high blood pressure, and it is not typically associated with a pudendal nerve block.
Option c) Fetal bradycardia is not a common adverse effect of a pudendal nerve block. Fetal bradycardia refers to a slow heart rate in the fetus. While fetal heart rate monitoring is important during labor, bradycardia is not typically associated with a pudendal nerve block.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today