A nurse is planning care for a newborn who is scheduled to start phototherapy using a lamp. Which of the following actions should the nurse include in the plan?
Give the newborn 1 oz of glucose water every 4 hours.
Apply a thin layer of lotion to the newborn's skin every 8 hours.
Ensure the newborn's eyes are closed beneath the shield.
Dress the newborn in a thin layer of clothing during therapy.
The Correct Answer is C
Phototherapy is a treatment method used to reduce high levels of bilirubin in the blood of a newborn with jaundice. During phototherapy, the newborn is exposed to special lights that help break down the bilirubin and allow it to be eliminated from the body. It is important to protect the newborn's eyes during phototherapy.
Option a) Giving the newborn 1 oz of glucose water every 4 hours is not necessary for phototherapy. The primary goal of phototherapy is to treat jaundice, and providing glucose water is not directly related to this treatment.
Option b)Applying a thin layer of lotion to the newborn's skin every 8 hours is not necessary during phototherapy. In fact, it is generally recommended to avoid applying lotions or oils to the skin during phototherapy as they can interfere with the effectiveness of the treatment.
Option c) Ensuring the newborn's eyes are closed beneath the shield is essential during phototherapy. The eyes are particularly sensitive to the light used in phototherapy, and exposure to the light can potentially damage the eyes. Therefore, the newborn's eyes should be protected with a shield or eye patches to prevent direct exposure to the light.
Option d) Dressing the newborn in a thin layer of clothing during therapy is appropriate. The newborn should be dressed in a way that allows as much of their skin as possible to be exposed to the phototherapy lights. This usually involves removing unnecessary clothing and covering the genital area with a diaper, while the rest of the body is exposed to the light.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
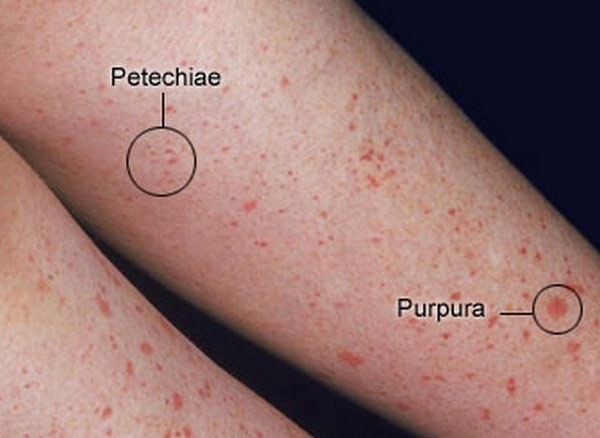
Facial petechiae are small, red or purple spots of bleeding under the skin or mucous membranes of the face. They are caused by the rupture of tiny blood vessels called capillaries. Facial petechiae can occur as a result of prolonged straining, such as during childbirth, vomiting, coughing, or crying¹. The increased pressure in the veins of the head and neck can cause the capillaries to burst, resulting in petechiae. Facial petechiae are usually harmless and resolve on their own without treatment.
The other options are not related to prolonged straining and have different causes and appearances:
a) Periauricular papillomas are benign, wart-like growths that occur near the ear. They are caused by human papillomavirus (HPV) infection and may be present at birth or develop later in life. They are usually painless and do not bleed⁴.
b) Erythema toxicum is a common skin condition in newborn babies. It causes a rash and small, fluid-filled bumps that may appear on the face, limbs, or chest. It is not caused by bleeding, infection, or allergy, but by an unknown mechanism. It does not cause discomfort to the baby and clears up without treatment within one to two weeks⁵.
d) Telangiectatic nevi are birthmarks that are caused by dilated blood vessels near the surface of the skin. They appear as red or purple patches or patterns on the skin that do not fade with pressure. They are present at birth and may grow in proportion to the child's growth. They are not associated with bleeding or infection and do not require treatment unless they cause cosmetic concerns⁶.
Correct Answer is C
Explanation
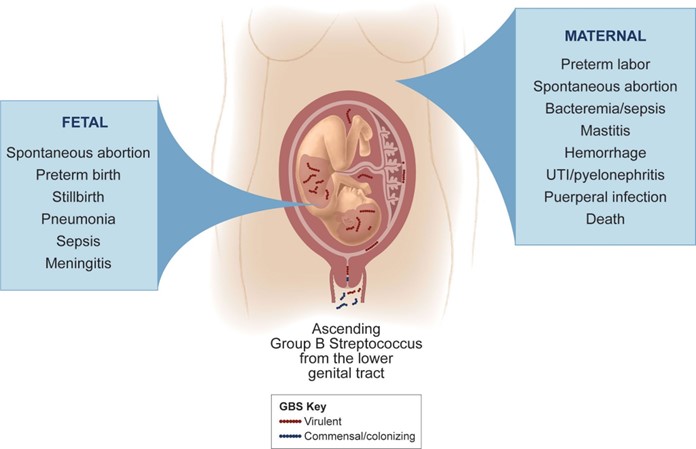
Group B Streptococcus β-hemolytic (GBS) is a type of bacteria that can cause serious infections in newborns, such as sepsis, pneumonia, and meningitis. GBS can be transmitted from the mother to the baby during labor and delivery if the mother is colonized with GBS in her vagina or rectum¹.
To prevent GBS infection in newborns, pregnant women who test positive for GBS or have risk factors for GBS should receive intravenous (IV) antibiotics during labor. The antibiotics can reduce the amount of GBS bacteria in the mother's body and lower the chance of passing them to the baby¹².
The recommended antibiotic for GBS prophylaxis is penicillin, which is safe and effective for most women. However, some women may be allergic to penicillin and need an alternative antibiotic. Ampicillin is one of the alternative antibiotics that can be used for GBS prophylaxis in women who have a mild allergy to penicillin (such as rash or itching). Ampicillin is also a type of penicillin, but it has a slightly different structure and may not cause an allergic reaction in some people²³.
Therefore, the nurse should plan to administer ampicillin to the client who tested positive for GBS and has a mild allergy to penicillin. The nurse should also monitor the client for any signs of anaphylaxis (a severe allergic reaction) and have epinephrine ready in case of emergency²³.
The other options are not medications that the nurse should administer to the client:
- a) Cefotetan is another alternative antibiotic that can be used for GBS prophylaxis in women who have a severe allergy to penicillin (such as anaphylaxis or angioedema). However, it is not indicated for women who have a mild allergy to penicillin, as it may still cause cross-reactivity and an allergic reaction²³.
- b) Fluconazole is an antifungal medication that is used to treat fungal infections, such as candidiasis (thrush) or cryptococcal meningitis. It is not effective against bacterial infections, such as GBS, and it is not indicated for GBS prophylaxis⁴.
- d) Doxycycline is an antibiotic that is used to treat bacterial infections, such as chlamydia, gonorrhea, or Lyme disease. It is not effective against GBS and it is not indicated for GBS prophylaxis. Moreover, doxycycline is contraindicated in pregnancy, as it can cause harm to the fetus, such as tooth discoloration or bone growth problems.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today