A nurse is planning care for a full-term newborn who is receiving phototherapy. Which of the following actions should the nurse include in the plan of care?
Keep the newborn supine throughout treatment.
Dress the newborn in lightweight clothing.
Measure the newborn's temperature every 8 hours.
Avoid using lotion or ointment on the newborn's skin.
The Correct Answer is D
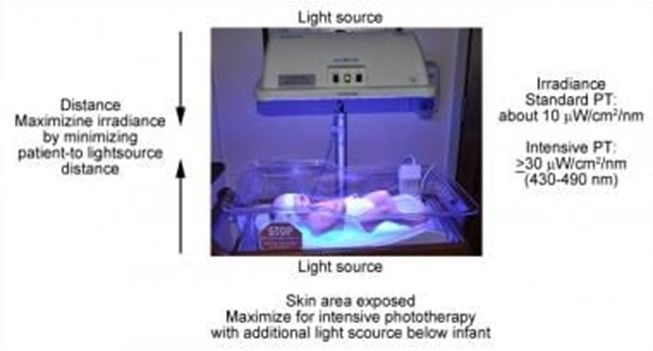
Phototherapy is a treatment that uses light to lower the level of bilirubin in the blood of newborns who have jaundice. Jaundice is a condition that causes yellowing of the skin and eyes due to high levels of bilirubin, a waste product that is normally removed by the liver. Phototherapy helps the body break down and eliminate bilirubin through urine and stool¹.
Phototherapy can be done at home or in the hospital, depending on the severity of jaundice and the type of light used. The most common types of light are fluorescent lamps, halogen lamps, or light-emitting diodes (LEDs). The light can be delivered through overhead units, fiber-optic blankets, or fiber-optic pads. The light should cover as much of the newborn's skin as possible, except for the eyes and genitals¹².
The nurse should follow certain guidelines when caring for a newborn who is receiving phototherapy, such
as:
- Monitor the newborn's temperature, hydration, weight, and urine and stool output regularly
- Protect the newborn's eyes with eye patches or goggles to prevent eye damage
- Turn the newborn every 2 to 4 hours to expose different parts of the body to the light
- Feed the newborn frequently to prevent dehydration and promote bilirubin excretion
- Check the newborn's skin color and bilirubin level periodically to evaluate the effectiveness of
phototherapy
- Provide emotional support and education to the parents about jaundice and phototherapy
One of the important guidelines is to avoid using lotion or ointment on the newborn's skin during phototherapy. This is because lotion or ointment can block the light from reaching the skin and reduce the effectiveness of phototherapy. Lotion or ointment can also cause skin irritation, rash, or burns if they react with the light. The newborn's skin should be clean and dry before phototherapy¹²³.
The other options are not actions that the nurse should include in the plan of care:
- a) Keep the newborn supine throughout treatment. This is not correct because keeping the newborn in one position can limit the exposure of different parts of the body to the light and reduce the effectiveness of phototherapy. The nurse should turn the newborn every 2 to 4 hours to expose different parts of the body to the light¹².
- b) Dress the newborn in lightweight clothing. This is not correct because dressing the newborn in clothing can block the light from reaching the skin and reduce the effectiveness of phototherapy. The newborn should be undressed except for a diaper during phototherapy¹².
- c) Measure the newborn's temperature every 8 hours. This is not correct because measuring the newborn's temperature every 8 hours may not be frequent enough to detect any changes in temperature that may occur during phototherapy. Phototherapy can cause overheating or hypothermia in newborns, depending on the type and intensity of light used. The nurse should monitor the newborn's temperature more often, such as every 2 to 4 hours, and adjust the room temperature or use blankets as needed¹².
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
In a newborn, bluish discoloration of the hands and feet may indicate a condition called peripheral cyanosis, which suggests poor oxygenation. It is important to report this finding to the healthcare provider promptly, as it may indicate a respiratory or circulatory problem that requires immediate attention.
Option a) Overlapping of the cranial bones is a common finding in newborns due to the molding of the head during delivery. This is not a priority finding to report unless there are other signs of concern, such as abnormal head shape or signs of trauma.
Option b) Small, distended white sebaceous glands on the face are called milia and are a normal finding in newborns. They are not a priority finding to report and typically resolve on their own within a few weeks.
Option c) Forward and lateral positioning of the ears is a normal finding in a newborn and is not a priority to report. The ears may appear folded or positioned differently due to the pressure and positioning in the womb.
Correct Answer is B
Explanation
The correct answer is choice B. Single palmar creases.
Choice A rationale:
Rust-stained urine is typically due to urate crystals and is common in newborns. It usually resolves on its own and is not a cause for concern.
Choice B rationale:
Single palmar creases can be associated with certain genetic conditions, such as Down syndrome. This finding should be reported to the provider for further evaluation.
Choice C rationale:
Subconjunctival hemorrhage is a common finding in newborns due to the pressure changes during delivery. It usually resolves without intervention and is not typically a cause for concern.
Choice D rationale:
Transient circumoral cyanosis is often seen in newborns and can occur when the baby is crying or feeding. It usually resolves on its own and is not typically a cause for concern.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today