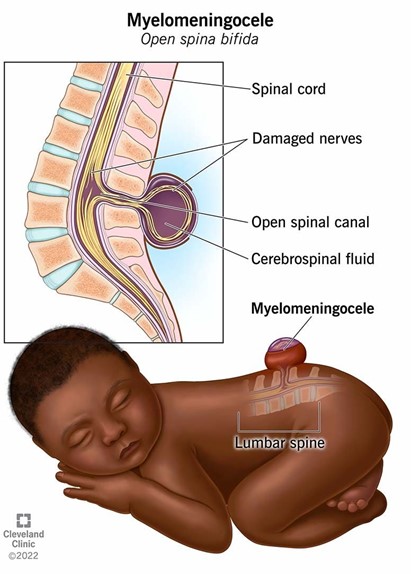
A nurse is planning care immediately following birth for a newborn who has a myelomeningocele that is leaking cerebrospinal fluid. Which of the following actions should the nurse include in the plan of care?
Cleanse the site with povidone-iodine.
Administer broad-spectrum antibiotics.
Prepare for surgical closure after 72 hours.
Monitor the rectal temperature every 4 hours.
The Correct Answer is B
A. Using povidone-iodine on the site of a myelomeningocele is not recommended as it can be irritating to the tissue and might not be safe for use on open neural tissue. The focus should be on preventing infection through other means.
B. Administering broad-spectrum antibiotics is crucial as the cerebrospinal fluid (CSF) leak increases the risk of infection, such as meningitis. Antibiotics help protect the newborn from potentially serious infections until surgical repair can be performed.
C. Surgical closure of a myelomeningocele is typically done as soon as possible, often within 24-48 hours after birth, to minimize the risk of infection and further damage to the exposed spinal cord.
D. While monitoring temperature is important, rectal temperature measurement is not recommended for a newborn with a myelomeningocele due to the risk of causing further complications. Axillary temperature measurement would be safer and less invasive.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
Breast development is a normal part of fetal and neonatal growth. It occurs in stages, starting before birth and continuing during puberty and adulthood. Breast development is influenced by hormones, such as estrogen and progesterone, that are produced by the ovaries or the placenta¹².
Breast development in newborns can vary depending on the gestational age, sex, weight, and exposure to maternal hormones. Some newborns may have palpable breast tissue at birth, while others may develop it later in the first weeks of life. Some newborns may also secrete milk from their breasts, which is called witch's milk or neonatal galactorrhea. This is a harmless and temporary phenomenon that usually resolves within a few weeks without treatment³⁴.
The degree of breast development in newborns can be assessed by using a scoring system that ranges from 0 to 5, based on the size of the areola (the dark area around the nipple) and the presence of a bud (a small lump of glandular tissue under the areola). The scoring system is as follows³:
- Score 0: No breast tissue; flat areola with no bud
- Score 1: Breast tissue < 5 mm; flat areola with no bud
- Score 2: Breast tissue 5 to 10 mm; flat areola with no bud
- Score 3: Breast tissue > 10 mm; raised areola with no bud
- Score 4: Breast tissue > 10 mm; raised areola with bud
- Score 5: Breast tissue > 10 mm; raised areola with large bud
The average score for term newborns is 2.5 for girls and 2.0 for boys. The score tends to be higher for heavier babies and lower for lighter babies. The score also tends to be higher for babies who were exposed to higher levels of maternal hormones during pregnancy, such as those whose mothers had diabetes, preeclampsia, or multiple gestation³⁴.
A score of 0 indicates that there is no breast tissue at all, and the areola is flat with no bud. This finding can indicate preterm gestational age, as breast development usually starts before birth and progresses with increasing gestational age. Preterm newborns may have delayed or incomplete breast development due to insufficient exposure to maternal hormones or immature development of their own hormonal system³⁵.
Therefore, the nurse should identify this finding as indicating preterm gestational age and monitor the newborn for any other signs of prematurity, such as low birth weight, small head size, thin skin, low body temperature, respiratory distress, or feeding difficulties. The nurse should also provide appropriate care and support to the newborn and the parents according to the hospital protocol³⁵.
- b) Ambiguous secondary sex characteristics are physical features that do not clearly match the typical male or female pattern, such as genitalia, hair distribution, or voice pitch. They can be caused by genetic disorders, hormonal imbalances, or environmental influences. Ambiguous secondary sex characteristics do not affect breast development in newborns, as breast tissue is present in both sexes and is influenced by maternal hormones rather than sex hormones¹ .
- c) Decreased maternal hormones during pregnancy can affect breast development in newborns, but not in the way described. Decreased maternal hormones during pregnancy can cause lower breast scores in newborns, as they may have less stimulation of their breast tissue from the placenta. However, this does not mean that they have no breast tissue at all or a flat areola with no bud. They may still have some degree of breast development depending on their gestational age, sex, weight, and exposure to their own hormones³⁴.
- d) Congenital anomaly is a term that refers to any structural or functional abnormality that is present at birth. Congenital anomalies can affect any part of the body and can have various causes, such as genetic mutations, chromosomal abnormalities, infections, drugs, or environmental factors. Congenital anomalies can affect breast development in newborns, but not in the way described. Congenital anomalies that affect breast development in newborns usually cause abnormal or absent nipples or breasts, such as nipple hypoplasia (underdeveloped nipples), athelia (absence of nipples), amastia (absence of breasts), or polymastia (extra breasts). These anomalies do not cause a flat areola with no bud .
Correct Answer is A
Explanation
After a client with eclampsia experiences a convulsion, the nurse should immediately prioritize ensuring adequate oxygenation for the client. Administering oxygen via a face mask at 10 L/min helps to increase oxygen levels and support the client's respiratory function. This intervention addresses the immediate need for oxygenation and helps support the client's respiratory function following a convulsion associated with eclampsia. Prompt and appropriate management of eclampsia is crucial to ensure the safety and well-being of both the mother and the fetus.
Option b) Placing the client in a Trendelenburg position (head down and legs elevated) is not appropriate in this situation. It can potentially worsen blood flow to the brain and may lead to increased intracranial pressure.
Option c) Assisting the client to void may be important for monitoring urine output, but it is not the immediate priority following a convulsion. The client's safety and stabilization take precedence.
Option d) Giving calcium gluconate is not indicated for the management of eclampsia. Calcium gluconate is used to treat hypocalcemia or as an antidote for certain medication toxicities. The primary treatment for eclampsia involves controlling and preventing seizures, which is not achieved through calcium gluconate administration.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today