A nurse midwife is examining a client who is primigravida at 42 weeks of gestation and states that she believes she is in labor. Which of the following findings confirm to the nurse that the client is in labor?
Amniotic fluid in the vaginal vault
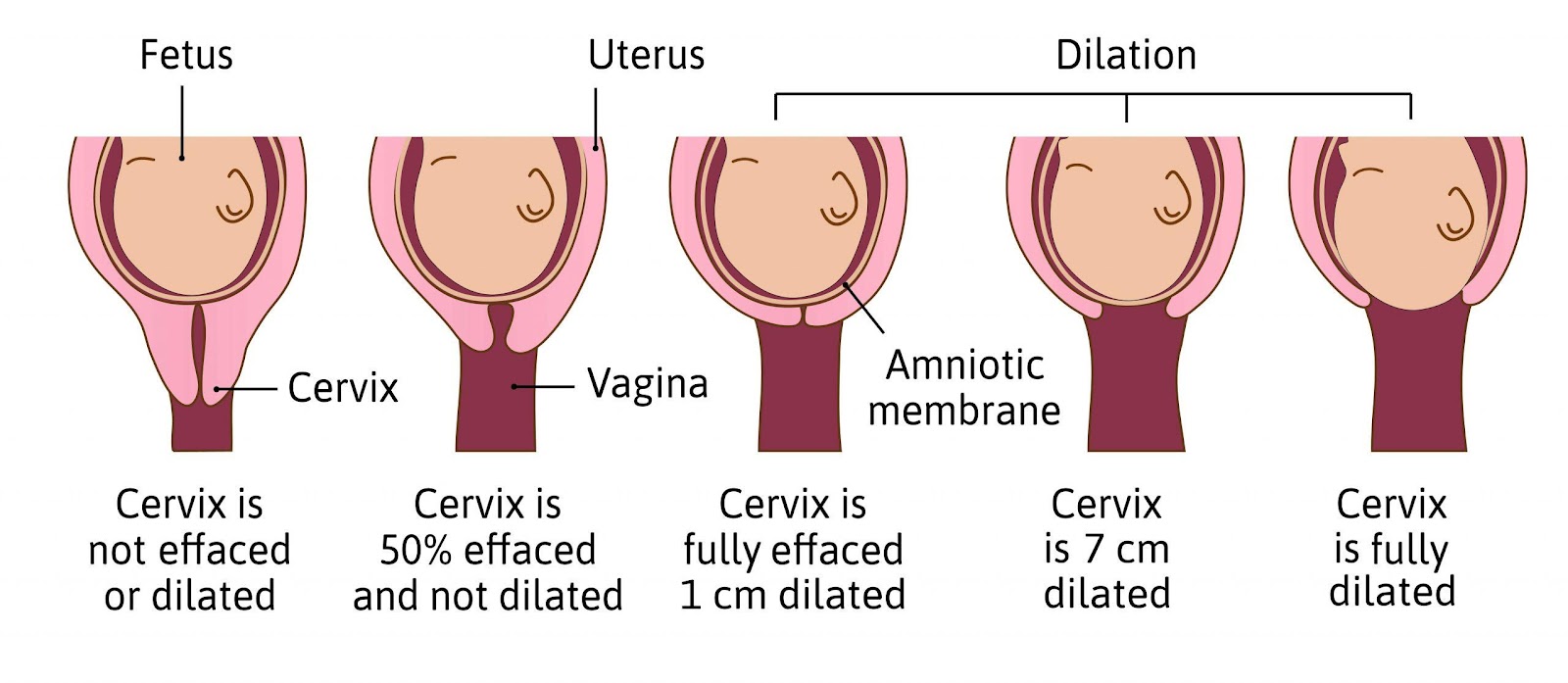
Cervical dilation
Brownish vaginal discharge
Report of pain above the umbilicus
The Correct Answer is B
Choice A rationale
Amniotic fluid in the vaginal vault is not a definitive sign of labor. It indicates that the membranes have ruptured, which can occur before or during labor. However, some clients may not have their membranes ruptured until the late stages of labor or during delivery.
Choice B rationale
Cervical dilation is a definitive sign of labor. It indicates that the cervix is opening and thinning to allow the passage of the fetus. Cervical dilation is measured in centimeters from 0 to 10, with 10 being fully dilated and ready for delivery.
Choice C rationale
Brownish vaginal discharge is not a definitive sign of labor. It may indicate the presence of the bloody show, which is the mucus plug that seals the cervix during pregnancy. The bloody show may be expelled before or during labor, but it does not necessarily mean that labor has started.
Choice D rationale
Report of pain above the umbilicus is not a definitive sign of labor. It may indicate the presence of Braxton Hicks contractions, which are irregular and painless contractions that occur throughout pregnancy. They are also known as false labor contractions, as they do not cause cervical dilation or effacement.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Choice A rationale
This is incorrect because repaglinide is not recommended for the treatment of gestational diabetes mellitus. Repaglinide is an oral antidiabetic agent that stimulates the release of insulin from the pancreas. However, it has not been adequately studied in pregnant women and may cause hypoglycemia or fetal harm.
Choice B rationale
This is correct because insulin is the preferred medication for the treatment of gestational diabetes mellitus. Insulin is a hormone that lowers the blood glucose levels by facilitating its uptake by the cells. Insulin does not cross the placenta and does not affect the fetal development. Insulin can be administered by injection or infusion, depending on the type and severity of the diabetes.
Choice C rationale
This is incorrect because glipizide is not recommended for the treatment of gestational diabetes mellitus. Glipizide is an oral antidiabetic agent that stimulates the release of insulin from the pancreas. However, it may cross the placenta and cause hypoglycemia or fetal abnormalities.
Choice D rationale
This is incorrect because acarbose is not recommended for the treatment of gestational diabetes mellitus. Acarbose is an oral antidiabetic agent that inhibits the digestion and absorption of carbohydrates in the intestine. However, it may cause gastrointestinal side effects, such as bloating, diarrhea, or flatulence, and it has not been proven to be safe or effective in pregnant women.
Correct Answer is D
Explanation
Choice A rationale
This is incorrect because the right upper quadrant is not the most likely location for fetal heart tones. The round, firm, movable part in the fundus of the uterus indicates that the fetal head is in the breech position. The long, smooth surface on the client's right side suggests that the fetal spine is on the same side. Therefore, the fetal heart tones would be best heard in the lower right quadrant, where the fetal chest is located.
Choice B rationale
This is incorrect because the left upper quadrant is not the most likely location for fetal heart tones. The round, firm, movable part in the fundus of the uterus indicates that the fetal head is in the breech position. The long, smooth surface on the client's right side suggests that the fetal spine is on the opposite side. Therefore, the fetal heart tones would be best heard in the lower right quadrant, where the fetal chest is located.
Choice C rationale
This is incorrect because the left lower quadrant is not the most likely location for fetal heart tones. The round, firm, movable part in the fundus of the uterus indicates that the fetal head is in the breech position. The long, smooth surface on the client's right side suggests that the fetal spine is on the opposite side. Therefore, the fetal heart tones would be best heard in the lower right quadrant, where the fetal chest is located.
Choice D rationale
This is correct because the right lower quadrant is the most likely location for fetal heart tones. The round, firm, movable part in the fundus of the uterus indicates that the fetal head is in the breech position. The long, smooth surface on the client's right side suggests that the fetal spine is on the same side. Therefore, the fetal heart tones would be best heard in the lower right quadrant, where the fetal chest is located.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today