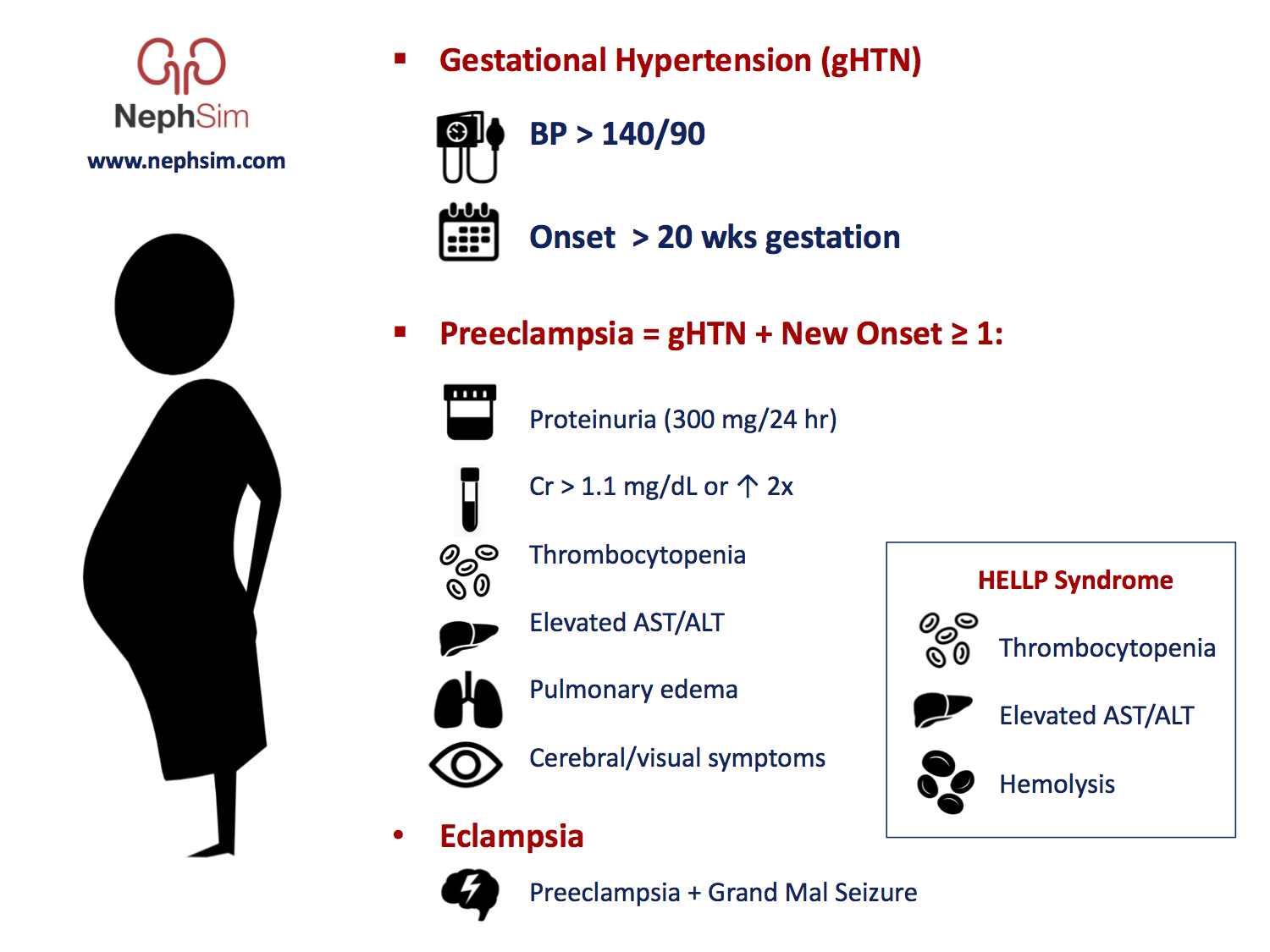
A nurse is caring for a client who is at 34 weeks of gestation. The client has a medical history of gestational diabetes, preeclampsia with previous pregnancy, and chronic hypertension for 5 years. The client's vital signs are: BP: 170/104 mm Hg, Pulse: 89/min, Respirations: 20/min, Temperature: 98.8°F (37.1°C) Oral, Oxygen saturation: 97% room air. The nurse is reviewing the client's medical record to develop a plan of care.
What are the two most important nursing interventions for this client?
Monitor the fetal heart rate and movement
Administer magnesium sulfate as prescribed
Encourage the client to drink plenty of fluids
Educate the client about the signs of preterm labor
The Correct Answer is A
Choice A rationale
Monitoring the fetal heart rate and movement is an important nursing intervention for this client. The client is at risk of fetal distress due to the high blood pressure, the preeclampsia, and the gestational diabetes. The fetal heart rate and movement can indicate the fetal well-being and oxygenation. The nurse should monitor the fetal heart rate continuously and perform a nonstress test or a biophysical profile as indicated.
Choice B rationale
Administering magnesium sulfate as prescribed is an important nursing intervention for this client. The client is at risk of seizures due to the severe preeclampsia. Magnesium sulfate is a medication that prevents and treats seizures in preeclamptic clients. The nurse should administer magnesium sulfate as prescribed and monitor the client's vital signs, reflexes, urine output, and magnesium level.
Choice C rationale
Encouraging the client to drink plenty of fluids is not an important nursing intervention for this client. The client is at risk of fluid overload due to the high blood pressure and the preeclampsia. Fluid overload can cause pulmonary edema, heart failure, and cerebral edema in the client. The nurse should restrict the client's fluid intake and monitor the client's weight, edema, and lung sounds.
Choice D rationale
Educating the client about the signs of preterm labor is not an important nursing intervention for this client. The client is at 34 weeks of gestation, which is close to the term pregnancy. The client is more likely to have a planned delivery or an induction of labor due to the high-risk conditions. The nurse should educate the client about the signs of preeclampsia, such as headache, blurred vision, epigastric pain, and decreased urine output.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Choice A rationale
This is incorrect because a client who has missed a period and reports vaginal spotting is not the most urgent case. This could indicate a possible pregnancy or a menstrual irregularity, but it is not a life-threatening condition. The nurse should see this client after assessing the other clients.
Choice B rationale
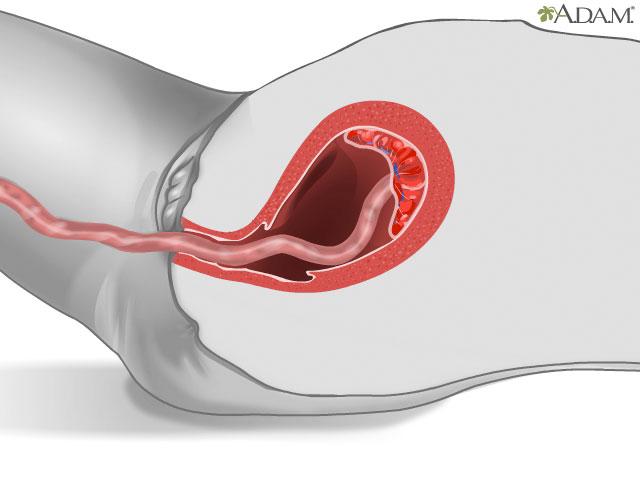
This is correct because a client who is at 28 weeks of gestation and reports painless vaginal bleeding is the most urgent case. This could indicate a placenta previa, which is a condition where the placenta covers the cervical opening and can cause severe hemorrhage and fetal distress. The nurse should see this client immediately and prepare for an emergency cesarean section.
Choice C rationale
This is incorrect because a client who is at 38 weeks of gestation and reports a cough and fever is not the most urgent case. This could indicate a respiratory infection, which can affect the maternal and fetal well-being, but it is not a life-threatening condition. The nurse should see this client after assessing the other clients and administer antibiotics and antipyretics as prescribed.
Choice D rationale
This is incorrect because a client who is at 14 weeks of gestation and reports nausea and vomiting is not the most urgent case. This could indicate a normal pregnancy symptom or a hyperemesis gravidarum, which is a condition where the nausea and vomiting are severe and persistent. The nurse should see this client after assessing the other clients and provide hydration and antiemetics as prescribed.
Correct Answer is C
Explanation
Choice A rationale
Assessing deep tendon reflexes every hour is an appropriate order for a client who has severe preeclampsia. This can help detect increased neuromuscular irritability, which is a sign of worsening preeclampsia or impending eclampsia. The nurse should report any hyperreflexia, clonus, or decreased sensation to the provider.
Choice B rationale
Continuous fetal monitoring is an appropriate order for a client who has severe preeclampsia. This can help assess the fetal well-being and detect any signs of fetal distress, such as bradycardia, tachycardia, or decreased variability. The nurse should report any abnormal fetal heart rate patterns to the provider.
Choice C rationale
Ambulating twice daily is not an appropriate order for a client who has severe preeclampsia. This may increase the risk of bleeding, seizures, or placental abruption. The client should be on bed rest or restricted activity to reduce the blood pressure and prevent complications.
Choice D rationale
Obtaining a daily weight is an appropriate order for a client who has severe preeclampsia. This can help monitor the fluid status and the severity of edema, which are common manifestations of preeclampsia. The nurse should report any excessive weight gain or loss to the provider.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today