A nurse is reviewing the medical record of a client who is 1-day post- operative following an appendectomy. Which of the following findings should the nurse report to the provider?
WBC count 8.400/mm3
Serosanguineous exudate noted on dressing change
Reports pain of 4 on a scale from 0 to 10 when coughing
Hemoglobin 10 mg/dL
The Correct Answer is D
Choice A reason:
WBC count 8,400/mm3 is not appropriate. This white blood cell count is within the normal range and is not a cause for concern.
Choice B reason:
Serosanguineous exudate noted on dressing change is not appropriate. Serosanguineous drainage is a normal finding in the early stages of wound healing and is expected after surgery.
Choice C reason:
Reports pain of 4 on a scale from 0 to 10 when coughing is not appropriate. A pain level of 4 out of 10 with coughing is a common and expected finding following an appendectomy. It's important for the nurse to assess and manage pain, but this is not an urgent concern.
Choice D reason:
Haemoglobin 10 mg/dL is appropriate. Haemoglobin level of 10 mg/dL indicates a low level of haemoglobin, which might suggest anaemia or blood loss. Reporting this finding to the provider is important as it could indicate a need for further evaluation or intervention.

Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Choice A reason:
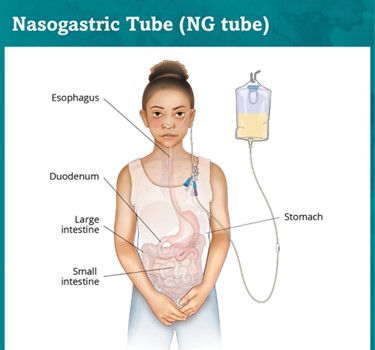
75 mL of greenish-yellow drainage should not be reported. This could be stomach contents or bile, which can be expected after surgery and might not be alarming.
Choice B reason:
150 mL of serosanguineous drainage should not be reported. Serosanguineous drainage is a mix of clear and slightly bloody fluid, which can be expected after surgery and may not be alarming.
Choice C reason:
100 mL of red drainage should be reported. After abdominal surgery, the drainage from an NG (nasogastric) tube is monitored to assess the client's condition and the status of their gastrointestinal system. Red drainage could indicate bleeding, which is a significant concern after surgery. The nurse should report this finding to the provider for further evaluation and intervention.
Choice D reason:
200 mL of brown drainage should not be reported. Brown drainage could also be indicative of old blood or digestive fluids, which might be expected after surgery and may not be alarming.
Correct Answer is C
Explanation
Administering the unit of packed RBCs over 1 hour is not appropriate. Packed RBCs are usually administered over a longer period of time (typically 2 to 4 hours), as rapid infusion can lead to adverse reactions. The rate of administration should be based on institutional policy.
Choice B Reason:
Initiating venous access with a 21-gauge needle is not appropriate-. The needle size for venous access can vary based on the client's condition and the size of their veins. However, a larger gauge needle (e.g., 18-gauge or 20-gauge) is typically used for blood transfusions to ensure adequate flow.
Choice C Reason:
Blood products should be infused through administration sets designed specifcally for blood; use a Y-tubing or straight-tubing blood administration set that contains a filter designed to trap fibrin clots and other debris that accumulate during blood storage.
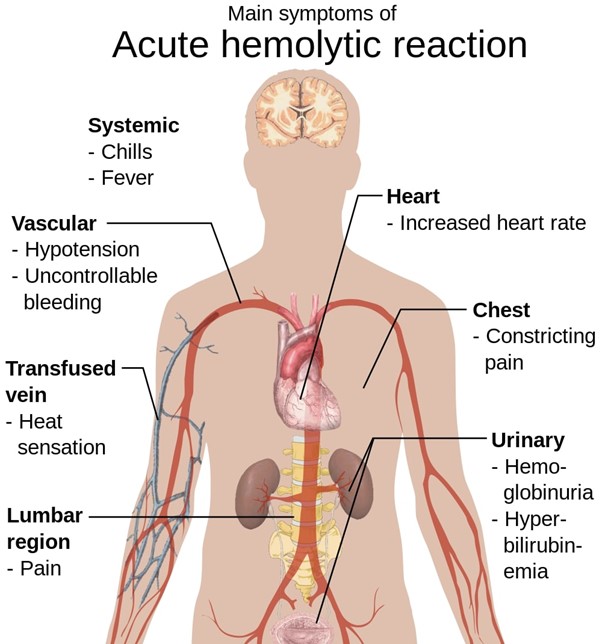
Choice D Reason:
The nurse should measure vital signs and assess lung sounds before the transfusion and again after the first 15 minutes and every 30 minutes to 1 hour (per agency policy) until 1 hour after the transfusion is completed.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today