A nurse is reinforcing teaching with a new mother about facility security measures. Which of the following statements by the mother indicates an understanding of the teaching?
“I can remove my security band to give it to a family member."
“I will have an identification band that matches the one my baby wears.”
“I can take my baby to the lobby to visit family."
“I will carry my baby to the nursery."
The Correct Answer is B
This statement shows that the mother understands the importance of having matching identification bands for herself and her baby. Matching identification bands help ensure proper identification and prevent any mix-ups or unauthorized individuals from gaining access to the baby. It is a security measure commonly implemented in healthcare facilities to protect the well-being and safety of both the mother and the newborn.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
When a nurse encounters a client who has fallen, the immediate priority is to assess the client's condition and ensure their safety. By measuring the client's vital signs, the nurse can gather important information about the client's overall well-being, such as heart rate, blood pressure, respiratory rate, and oxygen saturation. This assessment helps determine if there are any immediate medical concerns resulting from the fall, such as injury or shock, that require prompt attention.
The other options listed are also important but should be addressed after the initial assessment and safety measures:
- Notify the client's provider: After assessing the client's condition, if there are significant injuries or concerns identified, the nurse should promptly notify the client's provider to seek further medical guidance and intervention.
- Complete an incident report: Reporting the fall incident is an essential part of ensuring quality and safety in healthcare. However, it is not the first action the nurse should take. The immediate focus should be on the client's assessment and safety. Completing an incident report can be done once the client's immediate needs are addressed.
- Document the fall in the client's medical record: Documenting the fall in the client's medical record is important for maintaining accurate and comprehensive documentation. However, it should be done after the client's assessment, vital sign measurement, and any necessary interventions have been carried out.
Correct Answer is D
Explanation
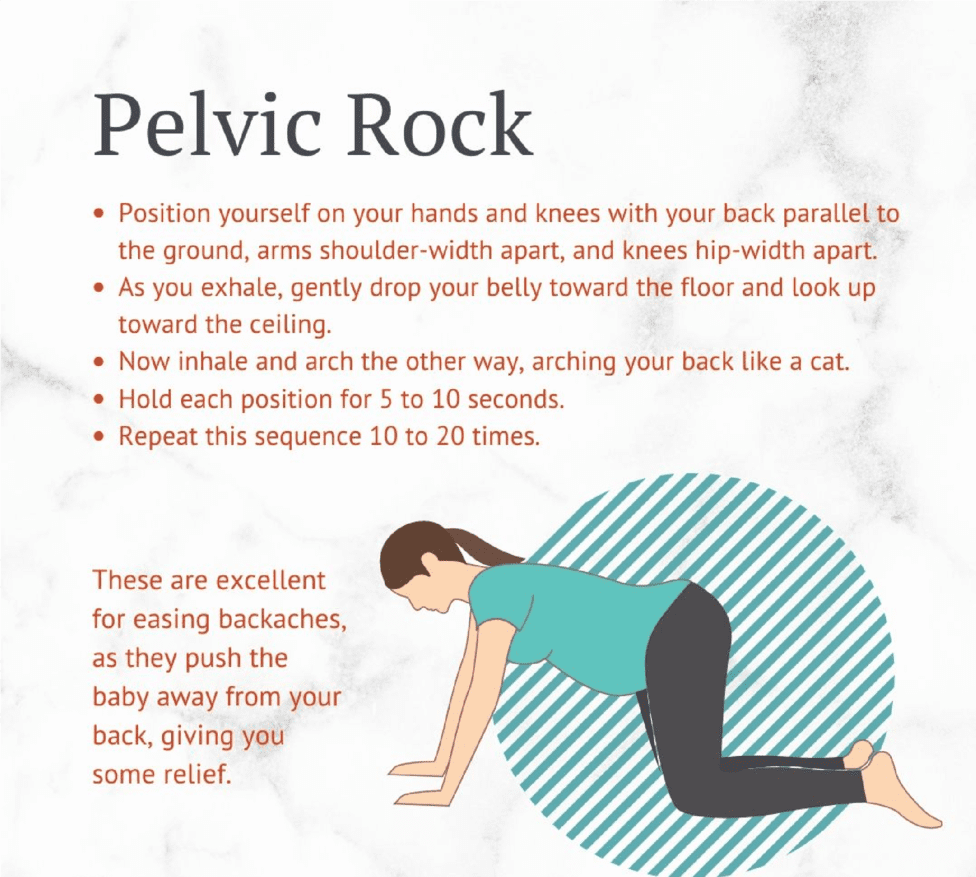
Pelvic rocking exercises can help relieve lower back pain during pregnancy. The client can perform this exercise by getting on their hands and knees, keeping their back straight, and gently rocking their pelvis back and forth. This helps to stretch and strengthen the muscles in the lower back and pelvis.
Sit in a hot tub for 30 min every evening: Hot tubs and hot baths are not recommended during pregnancy as they can raise the body temperature too high, which can be harmful to the developing fetus.
Raise chairs to keep knees lower than hips: This recommendation is more appropriate for promoting good posture and reducing strain on the back, but it may not specifically address lower back pain.
Use the arms to pick up heavy items: It is important to avoid heavy lifting during pregnancy as it can strain the back and increase the risk of injury. It is recommended to use proper lifting techniques, such as bending the knees and using the leg muscles rather than the back muscles, to lift objects.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today