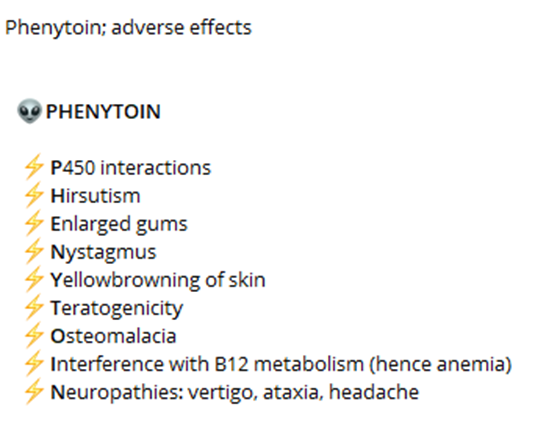
A nurse is reinforcing teaching a client who has a new prescription for phenytoin. The nurse should instruct the client to monitor and report which of the following adverse effects of this medication?
Diarrhea
Wrist pain
Skin rash
Metallic taste
The Correct Answer is C
A. Diarrhea:
Diarrhea is not a common side effect of phenytoin. While gastrointestinal disturbances such as nausea, vomiting, and constipation may occur, diarrhea is less common. Therefore, it is not a primary adverse effect that the nurse should instruct the client to monitor and report.
B. Wrist pain:
Wrist pain is not a common side effect of phenytoin. Side effects related to musculoskeletal issues such as joint pain, muscle weakness, or muscle twitching can occur, but wrist pain specifically is not commonly associated with phenytoin use. Therefore, it is not a primary adverse effect that the nurse should instruct the client to monitor and report.
C. Skin rash:
Skin rash is a potential adverse effect of phenytoin that should be monitored and reported. Phenytoin can cause various skin reactions, including a mild rash or more severe reactions such as Stevens-Johnson syndrome or toxic epidermal necrolysis. Therefore, the nurse should instruct the client to promptly report any signs of skin rash or other skin changes.
D. Metallic taste:
Metallic taste is a common side effect of phenytoin. While it is not usually a serious adverse effect, it can be bothersome for some individuals. Therefore, the nurse should instruct the client to monitor for this side effect and report it if it occurs persistently or becomes bothersome.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
A. Hyperglycemia:
Hyperglycemia refers to high blood sugar levels. While certain medications can affect glucose metabolism and potentially lead to hyperglycemia as a side effect, this is not typically associated with hydantoin therapy for seizure disorder. Therefore, it is less likely for the patient to experience hyperglycemia as a direct result of taking hydantoin medication.
B. Hunger:
Hunger is not a common side effect of hydantoin therapy for seizure disorder. While some medications may affect appetite or cause changes in eating habits, hunger is not a typical side effect of hydantoin medications such as phenytoin.
C. Hypoglycemia:
Hypoglycemia refers to low blood sugar levels, which can lead to symptoms such as confusion, dizziness, sweating, and weakness. Hydantoin medications, particularly phenytoin, can affect glucose metabolism and increase the risk of hypoglycemia, especially in patients who already have diabetes or are prone to low blood sugar. Therefore, it is important for patients taking hydantoin therapy to monitor their blood sugar levels regularly and be aware of the signs and symptoms of hypoglycemia.
D. Pupil dilation:
Pupil dilation, or mydriasis, is not a common side effect of hydantoin therapy for seizure disorder. While certain medications may affect pupil size, this is not typically associated with hydantoin medications such as phenytoin.
Correct Answer is C
Explanation
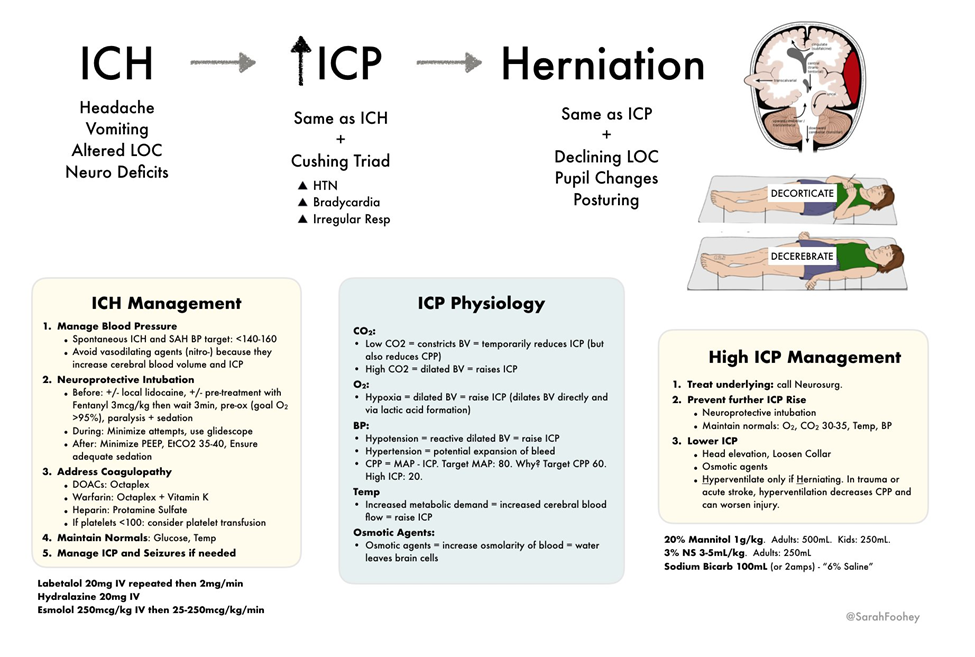
A. Instruct the client to perform controlled coughing and deep breathing.
This intervention is not appropriate for a client with increased intracranial pressure. Controlled coughing and deep breathing can increase intrathoracic pressure, which can in turn increase intracranial pressure. Therefore, this intervention should be avoided in clients with increased ICP.
B. Provide a brightly lit environment.
This intervention is not appropriate for a client with increased intracranial pressure. Bright lights can stimulate the reticular activating system and increase arousal, potentially exacerbating cerebral metabolic demand and intracranial pressure. Therefore, it is recommended to provide a calm, quiet environment with subdued lighting for clients with increased ICP.
C. Elevate the head of the bed 30°.
This intervention is correct. Elevating the head of the bed to 30 degrees promotes venous drainage from the head and reduces intracranial pressure. It helps prevent venous congestion in the brain and improves cerebral perfusion. This position is commonly used in clients with increased intracranial pressure to optimize cerebral blood flow.
D. Encourage a minimum intake of 2,000 mL/day of clear fluids.
This intervention is not appropriate for a client with increased intracranial pressure. While maintaining hydration is important for overall health, excessive fluid intake can increase intracranial pressure by increasing cerebral blood volume and cerebrospinal fluid production. Therefore, fluid intake should be carefully monitored and adjusted based on the client's condition and fluid balance.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today