A nurse is providing teaching to a client who has a new diagnosis of type 1 diabetes mellitus. The nurse should instruct the client to monitor for which of the following findings as a manifestation of hypoglycemia?
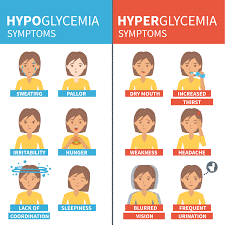
Irritability
Increased urination
Vomiting
Facial flushing
The Correct Answer is A
A. Irritability: Correct. Irritability is one of the signs of hypoglycemia, which occurs when blood glucose levels fall below 70 mg/dL (3.9 mmol/L). Other signs include shakiness, sweating, hunger, headache, confusion, and blurred vision.
B. Increased urination: Incorrect. Increased urination is one of the signs of hyperglycemia, which occurs when blood glucose levels rise above 180 mg/dL (10 mmol/L). Other signs include thirst, dry mouth, fatigue, nausea, and fruity breath odor.
C. Vomiting: Incorrect. Vomiting is not a specific sign of hypoglycemia or hyperglycemia, but it can occur as a complication of either condition if left untreated or poorly managed.
D.Facial flushing: Incorrect. Facial flushing is not a sign of hypoglycemia or hyperglycemia, but it can occur as a side effect of some medications used to treat diabetes, such as niacin or rosiglitazone.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
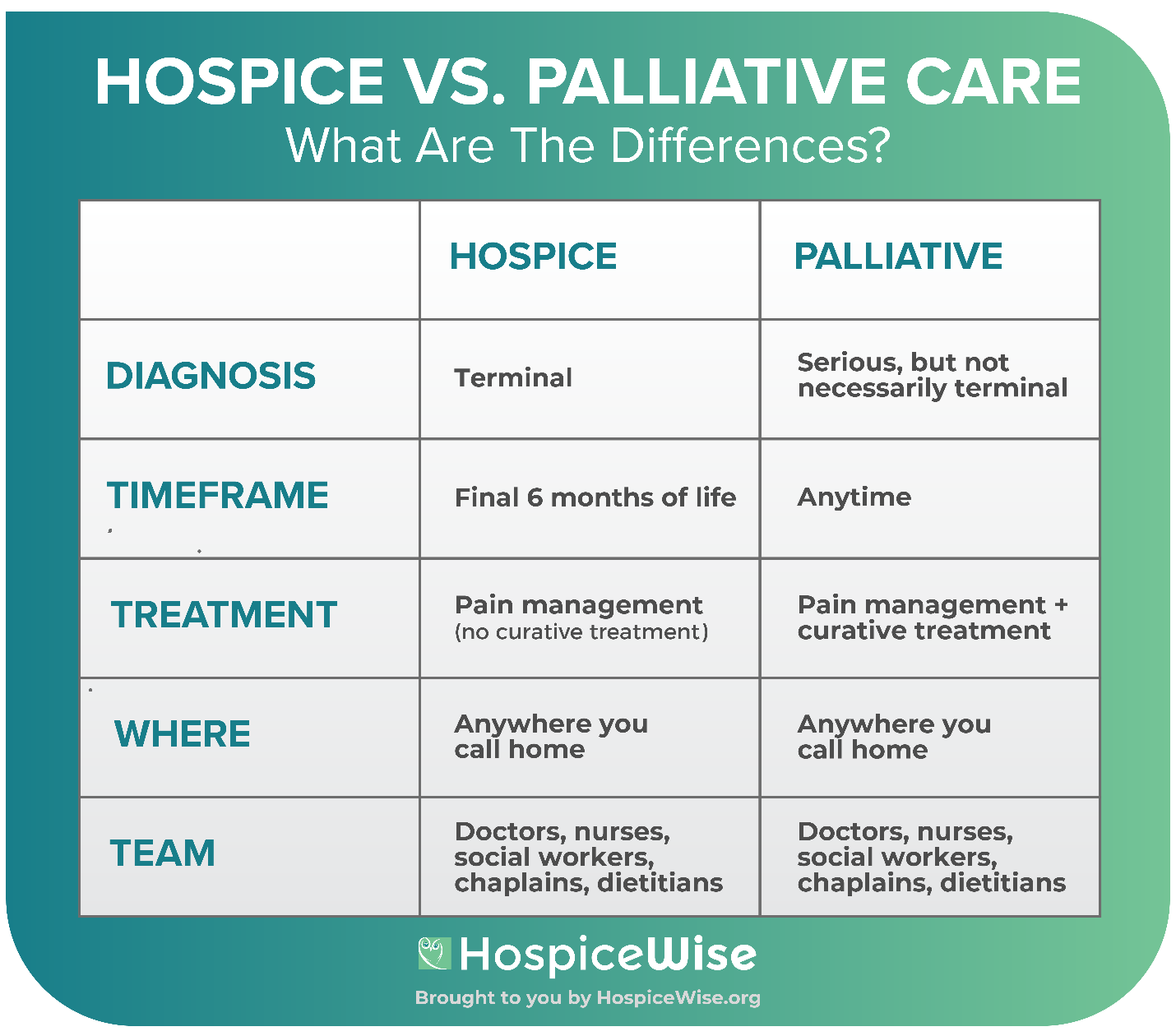
A is correct because hospice care includes bereavement support for the family for up to a year after the client's death.
B is incorrect because the hospice nurse does not administer pain medication, but rather teaches the family how to manage the client's pain at home.
C is incorrect because respite care is one of the services that hospice provides to allow the family to take a break from caregiving.
D is incorrect because hospice care does not aim to prolong life, but rather to provide comfort and quality of life for the client and the family.
Correct Answer is B
Explanation
A. Elevate the right leg above heart level. This is contraindicated for the adolescent because elevating the leg above heart level can increase blood pressure in the injured area and worsen bleeding and swelling.
B. Prepare the adolescent for surgery. This is anticipated for the adolescent because they have an open fracture with bone displacement, which requires surgical intervention to reduce the risk of infection and complications.
C. Remove the splint. This is contraindicated for the adolescent because removing the splint can cause further damage to the bone and soft tissues and increase pain and bleeding.
D. Apply ice to the affected extremity. This is contraindicated for the adolescent because applying ice can decrease blood flow to the injured area and impair healing and sensation.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today