A nurse is assessing a newborn's heart rate. Which of the following actions should the nurse take?
Assess the apical pulse while the newborn is crying.
Palpate the radial pulse for 30 seconds.
Listen to the apical pulse while palpating the radial pulse.
Auscultate the apical pulse at least 1 min.
The Correct Answer is D
A is incorrect because assessing the apical pulse while the newborn is crying can result in an inaccurate measurement due to increased heart rate and respiratory rate.
B is incorrect because palpating the radial pulse for 30 seconds is not appropriate for a newborn as it can be difficult to locate and count accurately.
C is incorrect because listening to the apical pulse while palpating the radial pulse is not necessary for a newborn and can be confusing and time-consuming.
D is correct because auscultating the apical pulse at least 1 min is the best way to assess a newborn's heart rate as it provides an accurate and reliable measurement.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
A. The LPN and AP lower the side rails before lifting the client up in bed is incorrect. This is a safe practice that prevents injury to the client and staff by providing more space for movement and reducing the risk of falling.
B. Prior to lifting the client, the LPN and AP raise the bed to waist level is incorrect. This is a safe practice that prevents injury to the client and staff by reducing the need for bending and lifting.
C. The LPN and the AP grasp the client under his arms to lift him up in bed is correct. This is an unsafe practice that can cause injury to the client's shoulders, neck, and axillae by applying excessive pressure and friction. The LPN and AP should use a draw sheet or a mechanical lift device to move the client up in bed.
D. The LPN and the AP ask the client to flex his knees and push his heels into the bed as they lift is incorrect. This is a safe practice that encourages active participation from the client and reduces the workload for the staff by using leverage.
Correct Answer is ["A","B"]
Explanation
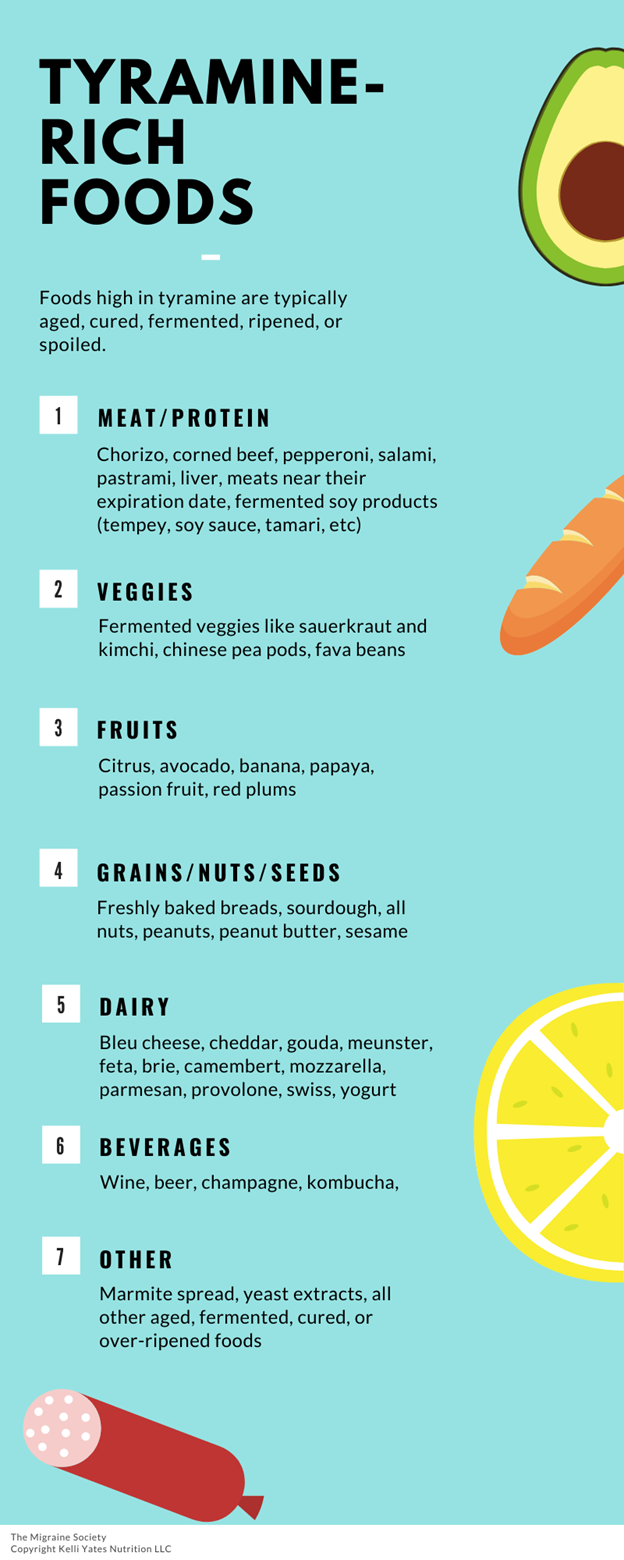
A: Correct. Broccoli is a vegetable that does not contain tyramine, which can interact with phenelzine and cause a hypertensive crisis.
B: Correct. Yogurt is a dairy product that does not contain tyramine, which can interact with phenelzine and cause a hypertensive crisis.
C: Incorrect. Pepperoni pizza contains pepperoni, cheese, and tomato sauce, which are all sources of tyramine, which can interact with phenelzine and cause a hypertensive crisis.
D: Incorrect. Cream cheese is a dairy product that contains tyramine, which can interact with phenelzine and cause a hypertensive crisis.
E: Incorrect. Bologna sandwich contains bologna, bread, and mayonnaise, which are all sources of tyramine, which can interact with phenelzine and cause a hypertensive crisis.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today