A nurse is prioritizing client care after receiving change-of-shift report. Which of the following clients should the nurse plan to see first?
A client who told an assistive personnel he is short of breath
A client who received oral pain medication 30 min ago
A client who is scheduled for an abdominal x-ray and is awaiting transport
A client who has a prescription for discharge
The Correct Answer is A
Choice A Reason: This is correct because a client who is short of breath is in immediate danger, as it indicates a possible respiratory compromise or failure. The nurse should assess the client's oxygen saturation, respiratory rate, and lung sounds, and provide oxygen therapy as needed.
Choice B Reason: This is incorrect because a client who received oral pain medication 30 min ago is not in immediate danger, as it indicates that the client's pain has been managed and the medication has had time to take effect.
Choice C Reason: This is incorrect because a client who is scheduled for an abdominal x-ray and is awaiting transport is not in immediate danger, as it indicates that the client's condition is stable and the diagnostic test is not urgent.
Choice D Reason: This is incorrect because a client who has a prescription for discharge is not in immediate danger, as it indicates that the client's condition has improved and the client is ready to leave the hospital.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
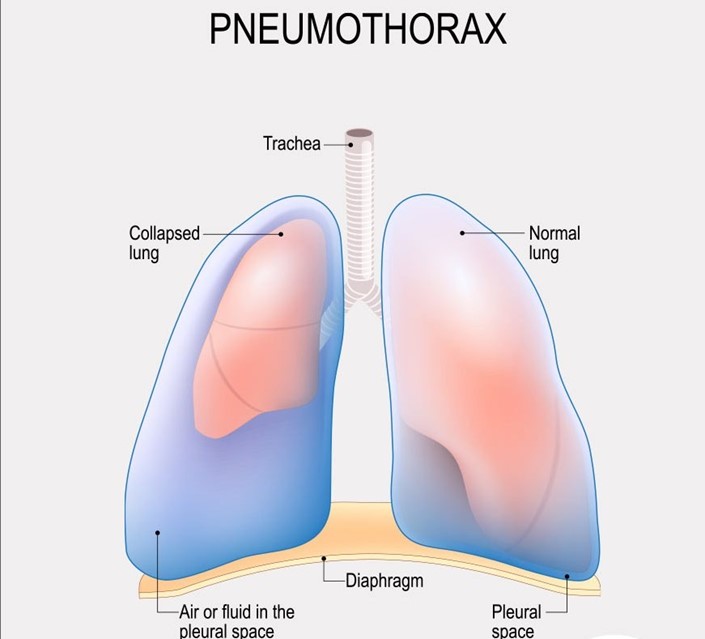
Choice A Reason: This is incorrect because crepitus in the area above and surrounding the insertion site is not a serious finding that requires notification of the provider. Crepitus is a crackling sensation that occurs when air leaks into the subcutaneous tissue. It is usually harmless and resolves on its own.
Choice B reason: This is incorrect because bubbling of the water in the water seal chamber with exhalation is a normal finding that indicates that air is being removed from the pleural space. Bubbling should stop when the pneumothorax is resolved.
Choice C Reason: This is incorrect because eyelets are not visible is not a serious finding that requires notification of the provider. Eyelets are small holes at the end of the chest tube that allow air and fluid to drain from the pleural space. They are usually covered by a dressing and may not be visible.
Choice D Reason: This is correct because movement of the trachea toward the unaffected side is a serious finding that indicates a tension pneumothorax, which is a life-threatening condition that occurs when air accumulates in the pleural space and causes pressure on the mediastinum. The nurse should notify the provider immediately and prepare for needle decompression or chest tube insertion.
Correct Answer is C
Explanation
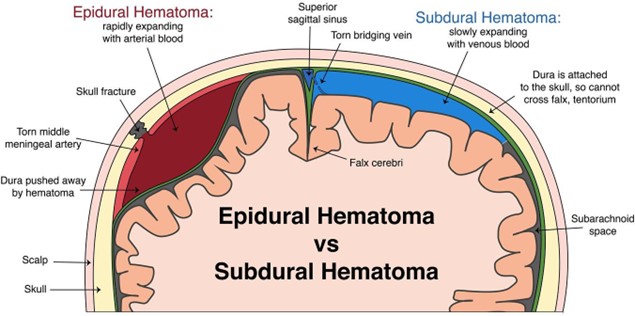
Choice A Reason: Albumin 25% is not a medication that the nurse should plan to administer for a client who is experiencing Cushing's triad following a subdural hematoma. Albumin 25% is a colloid solution that increases the oncotic pressure and draws fluid from the interstitial space into the intravascular space, which can worsen the intracranial pressure by increasing the cerebral blood flow and edema.
Choice B Reason: Dextran 70 is not a medication that the nurse should plan to administer for a client who is experiencing Cushing's triad following a subdural hematoma. Dextran 70 is a plasma expander that increases the blood volume and viscosity, which can also worsen the intracranial pressure by increasing the cerebral blood flow and edema.
Choice C Reason: Mannitol 25% is a medication that the nurse should plan to administer for a client who is experiencing Cushing's triad following a subdural hematoma. Mannitol 25% is an osmotic diuretic that reduces the intracranial pressure by creating an osmotic gradient and drawing fluid from the brain tissue into the blood vessels, which can then be excreted by the kidneys. The nurse should monitor the urine output, serum osmolality, and electrolytes when administering mannitol 25%.
Choice D Reason: Hydroxyethyl starch is not a medication that the nurse should plan to administer for a client who is experiencing Cushing's triad following a subdural hematoma. Hydroxyethyl starch is another plasma expander that has similar effects as dextran 70, and can also increase the risk of coagulopathy and renal failure.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today