A nurse is preparing to measure an infant's vital signs. The nurse should use which of the following sites to assess a heart rate?
Apex of the heart
Carotid artery
Brachial artery
Radial artery
The Correct Answer is A
A. Apex of the heart: The apex of the heart is the preferred site for measuring an infant's heart rate. It is located at the 4th or 5th intercostal space, just medial to the midclavicular line, allowing for accurate auscultation of the heartbeat.
B. Carotid artery: While the carotid artery can be used to assess heart rate in older children and adults, it is not ideal for infants due to the risk of compromising circulation to the brain if pressure is applied too forcefully.
C. Brachial artery: The brachial artery is often used to assess pulse in infants, especially in cases of CPR, but it is not the preferred site for routine heart rate measurement. It may be used when assessing circulation or checking for pulses, but auscultation at the apex is more accurate for heart rate.
D. Radial artery: The radial artery can be difficult to palpate in infants due to their small size and is generally not used for heart rate assessment in this age group. The apex is a more reliable location.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is ["260"]
Explanation
To calculate the total fluid intake, we need to convert all the measurements to milliliters (mL) and then add them up:
1 cup = 240 mL
1 oz = 30 mL
Given fluid intake:
Juice: ½ cup = 0.5 * 240 mL = 120 mL
Gelatin: 3 oz = 3 * 30 mL = 90 mL
Ice pop: 1 oz = 1 * 30 mL = 30 mL
Ginger ale: 20 mL
Total fluid intake = 120 mL + 90 mL + 30 mL + 20 mL = 260 mL
So, the nurse should record 260 mL as the child's fluid intake.
Correct Answer is A
Explanation
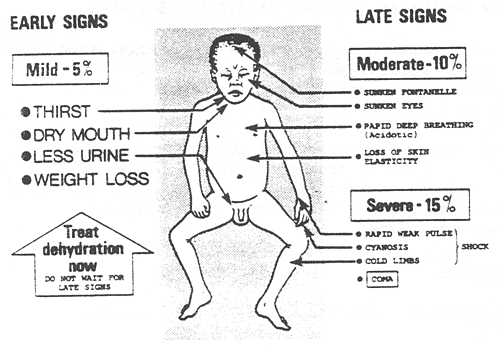
The nurse should expect to find irritability in an infant who is dehydrated. Dehydration in infants can lead to changes in behavior and irritability due to the imbalance in fluid and electrolytes. Other common signs of dehydration in infants may include:
Poor skin turgor (skin tenting)
Sunken fontanelles (soft spots on the baby's head)
Dry mucous membranes (dry mouth and tongue)
Decreased urine output or concentrated urine
Rapid heart rate (tachycardia)
Increased respiratory rate
Sunken eyes
Decreased tears when crying
B. Tetany is a condition characterized by involuntary muscle contractions and is more commonly associated with hypocalcemia (low calcium levels) rather than dehydration.
C. A slow, bounding pulse is not typically associated with dehydration. Dehydration often leads to a rapid heart rate (tachycardia) as the body attempts to compensate for the loss of fluid.
D. Decreased temperature is not a typical finding in dehydration. Dehydration can lead to fever in some cases due to an underlying infection, but it does not cause a decrease in body temperature on its own.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today