A nurse in an emergency department is assessing an infant who is dehydrated. Which of the following findings should the nurse expect?
Irritability
Tetany
slow, bounding pulse
Decreased temperature
The Correct Answer is A
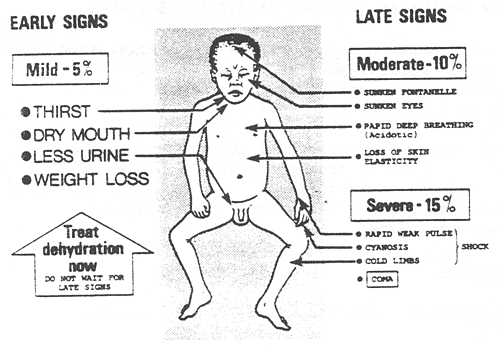
The nurse should expect to find irritability in an infant who is dehydrated. Dehydration in infants can lead to changes in behavior and irritability due to the imbalance in fluid and electrolytes. Other common signs of dehydration in infants may include:
Poor skin turgor (skin tenting)
Sunken fontanelles (soft spots on the baby's head)
Dry mucous membranes (dry mouth and tongue)
Decreased urine output or concentrated urine
Rapid heart rate (tachycardia)
Increased respiratory rate
Sunken eyes
Decreased tears when crying
B. Tetany is a condition characterized by involuntary muscle contractions and is more commonly associated with hypocalcemia (low calcium levels) rather than dehydration.
C. A slow, bounding pulse is not typically associated with dehydration. Dehydration often leads to a rapid heart rate (tachycardia) as the body attempts to compensate for the loss of fluid.
D. Decreased temperature is not a typical finding in dehydration. Dehydration can lead to fever in some cases due to an underlying infection, but it does not cause a decrease in body temperature on its own.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Severe anemia is a condition characterized by a significant decrease in the number of red blood cells or hemoglobin in the blood, leading to reduced oxygen-carrying capacity. This can result in fatigue, weakness, and shortness of breath in the affected individual.
A red blood cell transfusion is given to a child with severe anemia to increase the number of red blood cells and, consequently, the hemoglobin level in the blood. This helps improve oxygen delivery to tissues and organs, which can lead to increased energy levels and reduced fatigue.
Option A is incorrect because red blood cell transfusion is not given to help the body stop bleeding by forming a clot. Platelets are responsible for clot formation, not red blood cells.
Option B is incorrect because a red blood cell transfusion is not used to fight infections. White blood cells and the immune system are responsible for fighting infections.
Option D is incorrect because a red blood cell transfusion is not given to allow her parents to come to visit her. Transfusions are medical treatments to address specific medical conditions and are not related to visitation rights.
Correct Answer is D
Explanation
In cystic fibrosis, the pancreas does not secrete enough digestive enzymes, leading to malabsorption of nutrients, especially fats. To help with digestion, pancreatic enzymes are prescribed to be taken with meals and snacks. These enzymes should be given just before or with each meal or snack to aid in the breakdown and absorption of nutrients.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today