A nurse is performing an abdominal assessment on a client. Identify the sequence of actions the nurse should take.
Auscultation
Inspection
Palpation
Percussion
The Correct Answer is B, A, D, C
B. Inspection is the first step in an abdominal assessment because it allows the nurse to observe the shape, size, symmetry, contour, and movement of the abdomen. Inspection also helps to identify any abnormalities such as scars, lesions, masses, or distension.
A. Auscultation is the second step in an abdominal assessment because it allows the nurse to listen to the bowel sounds and vascular sounds of the abdomen. Auscultation should be performed before palpation or apercussion because these maneuvers could alter the sounds.
D. Percussion is the third step in an abdominal assessment because it allows the nurse to elicit sounds from different organs and structures in the abdomen. Percussion helps to determine the size, location, density, and consistency of the organs and to detect any fluid or air accumulation.
C. Palpation is the last step in an abdominal assessment because it allows the nurse to feel the texture, temperature, tenderness, and masses of the abdomen. Palpation should be performed gently and carefully to avoid causing pain or injury to the client.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is ["A","C","E","F"]
Explanation
A. This choice is correct because mental status changes, such as agitation, confusion, or delirium, are common signs of thyroid storm, which is a life-threatening complication of hyperthyroidism that occurs when there is excessive release of thyroid hormones.
B. This choice is incorrect because wound drainage is not a specific sign of thyroid storm, but rather a potential complication of any surgery that can indicate infection or bleeding.
C. This choice is correct because tachycardia, or increased heart rate, is a common sign of thyroid storm, which can result from increased metabolic demand and increased sensitivity to catecholamines.
D. This choice is incorrect because pain is not a specific sign of thyroid storm, but rather a common symptom of any surgery that can be managed with analgesics.
E. This choice is correct because hypertension, or increased blood pressure, is a common sign of thyroid storm, which can result from increased cardiac output and peripheral vascular resistance.
F. This choice is correct because hyperthermia, or increased temperature, is a common sign of thyroid storm, which can result from increased heat production and impaired heat dissipation.
Correct Answer is A
Explanation
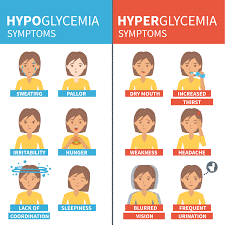
A. Irritability: Correct. Irritability is one of the signs of hypoglycemia, which occurs when blood glucose levels fall below 70 mg/dL (3.9 mmol/L). Other signs include shakiness, sweating, hunger, headache, confusion, and blurred vision.
B. Increased urination: Incorrect. Increased urination is one of the signs of hyperglycemia, which occurs when blood glucose levels rise above 180 mg/dL (10 mmol/L). Other signs include thirst, dry mouth, fatigue, nausea, and fruity breath odor.
C. Vomiting: Incorrect. Vomiting is not a specific sign of hypoglycemia or hyperglycemia, but it can occur as a complication of either condition if left untreated or poorly managed.
D.Facial flushing: Incorrect. Facial flushing is not a sign of hypoglycemia or hyperglycemia, but it can occur as a side effect of some medications used to treat diabetes, such as niacin or rosiglitazone.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today