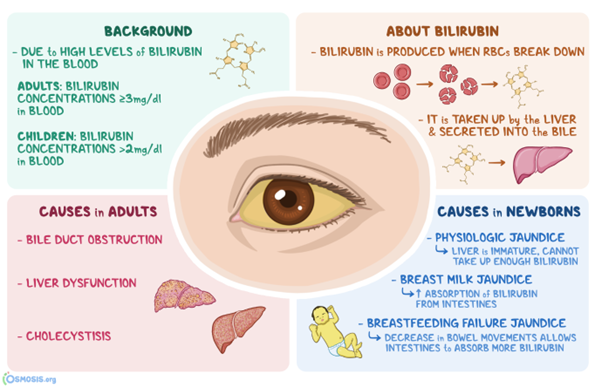
A nurse is performing a skin assessment on a client who has a dark skin. Which one of the following locations on the client’s body should the nurse observe to access for jaundice?
Face
Shoulders
Palm of the hands
Sclera
The Correct Answer is D
Choice A reason:
Face is incorrect: Facial skin colour can vary for many reasons, but it may not be the best indicator of jaundice in individuals with dark skin.
Choice B reason
Shoulders is incorrect: The shoulders are not typically indicative of jaundice.
Choice C reason:
Palm of the hands is incorrect: While the palm of the hands can sometimes show yellowing in cases of jaundice, it is less reliable than observing the sclera.
Choice D reason:
Sclera is the best location. In individuals with darker skin tones, yellowish discoloration of the skin due to jaundice can be more challenging to detect. However, the sclera of the eyes can still show noticeable yellowing, making it a reliable location for assessing jaundice in individuals with both light and dark skin.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is ["A","B"]
Explanation
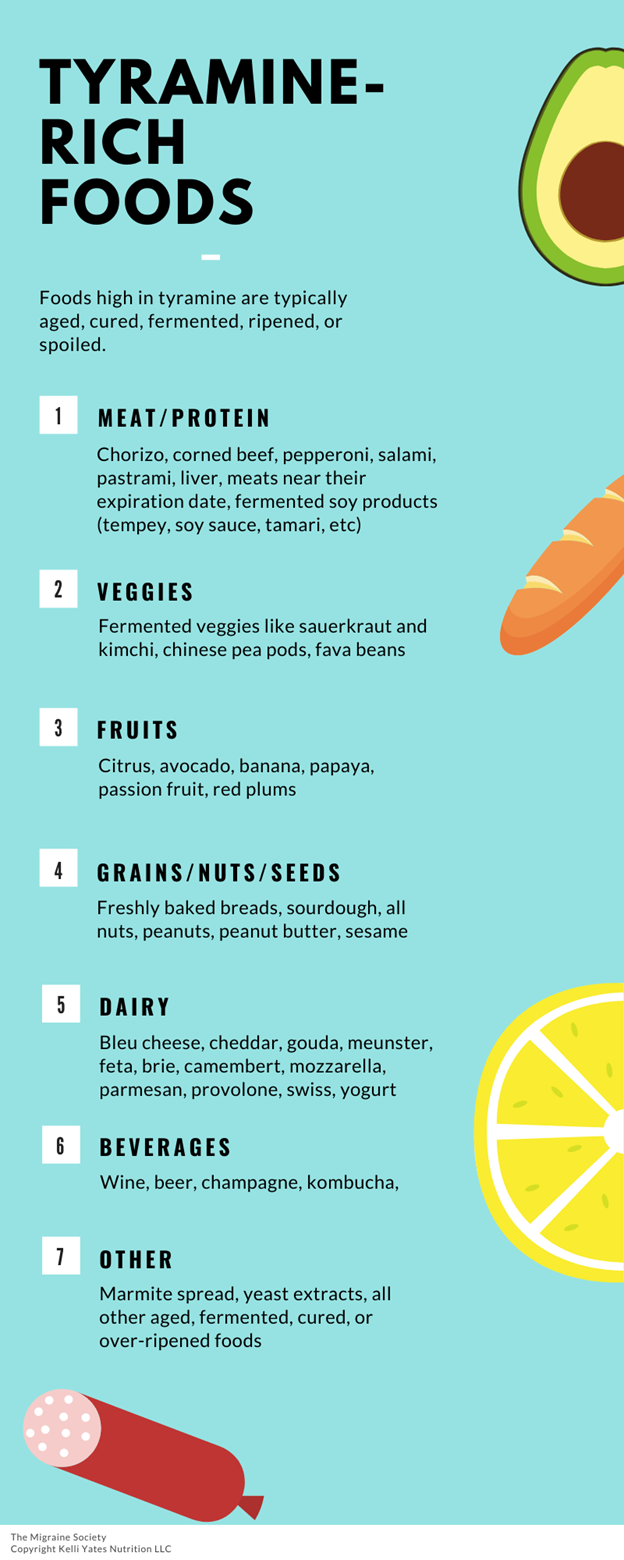
A: Correct. Broccoli is a vegetable that does not contain tyramine, which can interact with phenelzine and cause a hypertensive crisis.
B: Correct. Yogurt is a dairy product that does not contain tyramine, which can interact with phenelzine and cause a hypertensive crisis.
C: Incorrect. Pepperoni pizza contains pepperoni, cheese, and tomato sauce, which are all sources of tyramine, which can interact with phenelzine and cause a hypertensive crisis.
D: Incorrect. Cream cheese is a dairy product that contains tyramine, which can interact with phenelzine and cause a hypertensive crisis.
E: Incorrect. Bologna sandwich contains bologna, bread, and mayonnaise, which are all sources of tyramine, which can interact with phenelzine and cause a hypertensive crisis.
Correct Answer is D
Explanation
A. Discussing the suspicion of physical abuse with the provider isis essential, but it should not replace reporting to CPS. The provider’s input is valuable, but immediate action is necessary.
B. Confronting the parents with the suspicion of physical abuse is not an appropriate action for the nurse to take, as it can escalate the situation and endanger the child or the nurse.
C. Asking the hospital security to detain and question the parents is not an appropriate action for the nurse to take, as it violates the parents' rights and may interfere with the legal process.
D. Contacting Child Protective Servicesnurses are legally required to report all cases of suspected child abuse to the appropriate local or state agency.It's a critical step in protecting the child from further harm.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today