A nurse is monitoring an infant who is 6 months old and has sneezing, coughing, nasal congestion, intermittent fever, and apneic spells. The nurse should recognize these findings are consistent with which of the following diagnoses?
Epiglottitis
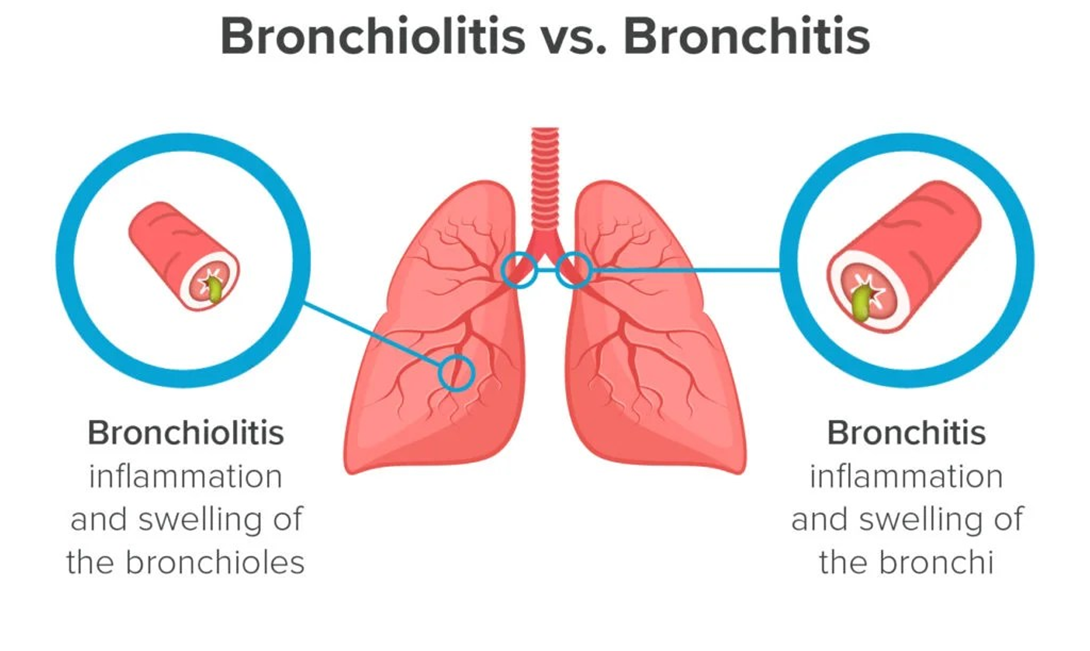
Bronchiolitis
Influenza
Croup
The Correct Answer is B
Choice A reason: Epiglottitis is a life-threatening condition that causes inflammation and swelling of the epiglottis, the flap of tissue that covers the entrance to the trachea. It can block the airway and cause respiratory distress. The signs and symptoms of epiglottitis include drooling, dysphagia, dysphonia, high fever, and tripod position. Epiglottitis is rare in infants and more common in children aged 2-6 years.
Choice B reason: Bronchiolitis is a viral infection that causes inflammation and mucus production in the bronchioles, the smallest airways in the lungs. It can impair gas exchange and cause respiratory distress. The signs and symptoms of bronchiolitis include sneezing, coughing, nasal congestion, wheezing, tachypnea, retractions, and apneic spells. Bronchiolitis is common in infants and children under 2 years of age, especially during the winter months.
Choice C reason: Influenza is a viral infection that affects the respiratory system. It can cause fever, chills, headache, muscle aches, fatigue, sore throat, cough, and nasal congestion. Influenza can also lead to complications such as pneumonia, otitis media, and sinusitis. Influenza is common in children and adults of all ages, especially during the flu season.
Choice D reason: Croup is a viral infection that causes inflammation and narrowing of the larynx and trachea. It can cause a characteristic barking cough, hoarseness, stridor, and respiratory distress. Croup is common in children aged 6 months to 3 years, especially during the fall and winter months.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
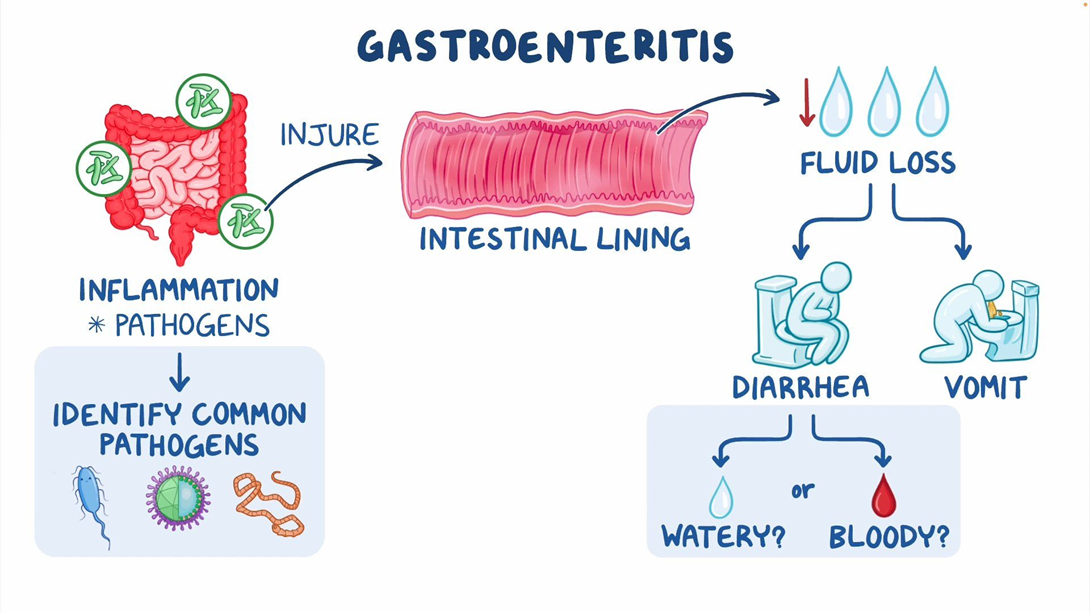
Choice A reason: Oral rehydration solution (ORS) is the best fluid for a child with acute gastroenteritis, as it contains the optimal balance of electrolytes and glucose to prevent dehydration and restore fluid balance. ORS is recommended by the World Health Organization (WHO) and the American Academy of Pediatrics (AAP) for the management of diarrhea in children.
Choice B reason: Water is not a good fluid for a child with acute gastroenteritis, as it does not contain any electrolytes or glucose and can dilute the blood sodium level, leading to hyponatremia. Water can also increase the osmotic load in the intestines and worsen diarrhea.
Choice C reason: Broth is not a good fluid for a child with acute gastroenteritis, as it is high in sodium and can cause hypernatremia and dehydration. Broth can also irritate the intestinal mucosa and increase diarrhea.
Choice D reason: Diluted apple juice is not a good fluid for a child with acute gastroenteritis, as it is high in fructose and can cause osmotic diarrhea. Apple juice can also lower the blood pH and cause metabolic acidosis.
Correct Answer is D
Explanation
Choice A reason: This statement is incorrect, as montelukast is a leukotriene receptor antagonist that is used for long-term control and prevention of asthma symptoms. It is not effective for acute asthma attacks, as it does not provide immediate bronchodilation.
Choice B reason: This statement is incorrect, as budesonide is an inhaled corticosteroid that is used for long-term control and prevention of inflammation in asthma. It is not effective for acute asthma attacks, as it does not provide immediate relief of bronchospasm.
Choice C reason: This statement is incorrect, as prednisone is an oral corticosteroid that is used for short-term treatment of severe asthma exacerbations. It is not effective for acute asthma attacks, as it takes several hours to exert its anti-inflammatory effect.
Choice D reason: This statement is correct, as albuterol is a short-acting beta2 agonist that is used for quick relief of acute asthma symptoms. It provides rapid bronchodilation by relaxing the smooth muscles of the airways.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today