A nurse is caring for a 6-week-old infant who has pyloric stenosis. Which of the following clinical manifestations should the nurse expect?
Distended neck veins
Rigid abdomen
Projectile vomiting
Red currant jelly stools
The Correct Answer is C
Choice A: Distended neck veins are not a clinical manifestation of pyloric stenosis, which is a condition that causes the narrowing of the pylorus, which is the opening between the stomach and the small intestine. Distended neck veins are a sign of increased venous pressure, which can occur in conditions that affect the right side of the heart or cause fluid overload.
Choice B: Rigid abdomen is not a clinical manifestation of pyloric stenosis, but rather a sign of peritonitis, which is inflammation of the peritoneum, which is the membrane that lines the abdominal cavity. Peritonitis can be caused by infection, perforation, or trauma to any abdominal organ. A rigid abdomen indicates severe pain and inflammation in the abdominal cavity.
Choice C: Projectile vomiting is a clinical manifestation of pyloric stenosis, as it indicates forceful expulsion of stomach contents due to obstruction at the pylorus. Projectile vomiting can occur shortly after feeding and may contain undigested milk or formula. Projectile vomiting can cause dehydration, electrolyte imbalance, or weight loss.
Choice D: Red currant jelly stools are not a clinical manifestation of pyloric stenosis, but rather a sign of intussusception, which is a condition that causes telescoping of one segment of bowel into another. Intussusception can cause obstruction and ischemia of the bowel and lead to bleeding and necrosis. Red currant jelly stools indicate blood and mucus in the stool.

Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
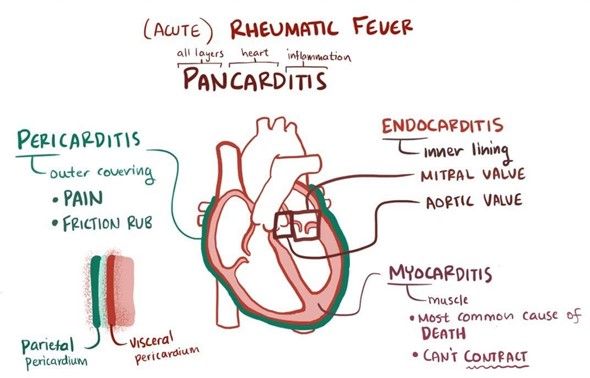
Choice A: Using a pain-rating tool to determine the severity of the joint pain is not the priority assessment for an 8-year-old child who has acute rheumatic fever, which is an inflammatory condition that can affect various organs, especially the heart, joints, skin, and brain. Joint pain is one of the major criteria for diagnosing acute rheumatic fever and can affect one or more large joints, such as knees, ankles, elbows, or wrists. Joint pain can be managed with analgesics or anti-inflammatory drugs.
Choice B: Assessing the client's erythematous rash is not the priority assessment for an 8-year-old child who has acute rheumatic fever, which is an inflammatory condition that can affect various organs, especially the heart, joints, skin, and brain. The erythematous rash is one of the minor criteria for diagnosing acute rheumatic fever and can appear as pink or red patches on the trunk or limbs. The erythematous rash can fade or change location over time and does not require any specific treatment.
Choice C: Identifying the degree of parental anxiety related to the diagnosis is not the priority assessment for an 8-year-old child who has acute rheumatic fever, which is an inflammatory condition that can affect various organs, especially the heart, joints, skin, and brain. Parental anxiety related to the diagnosis can affect their coping skills and ability to care for their child. Parental anxiety can be addressed by providing education, support, and referral to appropriate resources.
Choice D: Auscultating the rate and regularity of the child's heart sounds and notifying the provider immediately of abnormalities is the priority assessment for an 8-year-old child who has acute rheumatic fever, as it can indicate cardiac involvement, which is the most serious complication of acute rheumatic fever. Cardiac involvement can cause damage to the heart valves, myocardium, or pericardium and lead to heart failure or death. Abnormalities in heart sounds may include murmurs, rubs, gallops, or arrhythmias.
Correct Answer is A
Explanation
Choice A reason: This choice is correct because providing a latex-free environment is an essential intervention for an infant who has spina bifida and is to undergo surgical closure of the myelomeningocele sac. Spina bifida is a congenital defect in which the spinal cord and its coverings do not close properly, resulting in a protrusion of the meninges (meningocele) or the meninges and spinal cord (myelomeningocele). Children who have spina bifida are at a high risk of developing a latex allergy, which can cause severe reactions such as anaphylaxis or death. Therefore, avoiding exposure to latex products such as gloves, catheters, balloons, or bandages is crucial to prevent complications.
Choice B reason: This choice is incorrect because initiating contact precautions is not necessary for an infant who has spina bifida and is to undergo surgical closure of the myelomeningocele sac. Contact precautions are infection control measures that prevent the transmission of microorganisms that can be spread by direct or indirect contact with the client or their environment. They may be indicated for clients who have multidrug-resistant organisms, clostridium difficile, or scabies, but they are not required for clients who have spina bifida unless they have a concurrent infection.
Choice C reason: This choice is incorrect because limiting visitors to immediate family members is not indicated for an infant who has spina bifida and is to undergo surgical closure of the myelomeningocele sac. Limiting visitors may be indicated for clients who have immunosuppression, isolation, or terminal illness, but it may not be beneficial for clients who have spina bifida. Allowing visitors may provide emotional and social support for the client and their family, as long as they follow standard precautions and do not pose any risk of infection or injury.
Choice D reason: This choice is incorrect because maintaining the infant in the supine position is not an appropriate intervention for an infant who has spina bifida and is to undergo surgical closure of the myelomeningocele sac.
Maintaining the infant in the supine position may cause pressure or trauma to the sac, which can lead to rupture, infection, or nerve damage. Therefore, positioning the infant in a prone or side-lying position with the hips flexed and knees abducted can help to protect the sac and prevent complications.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today