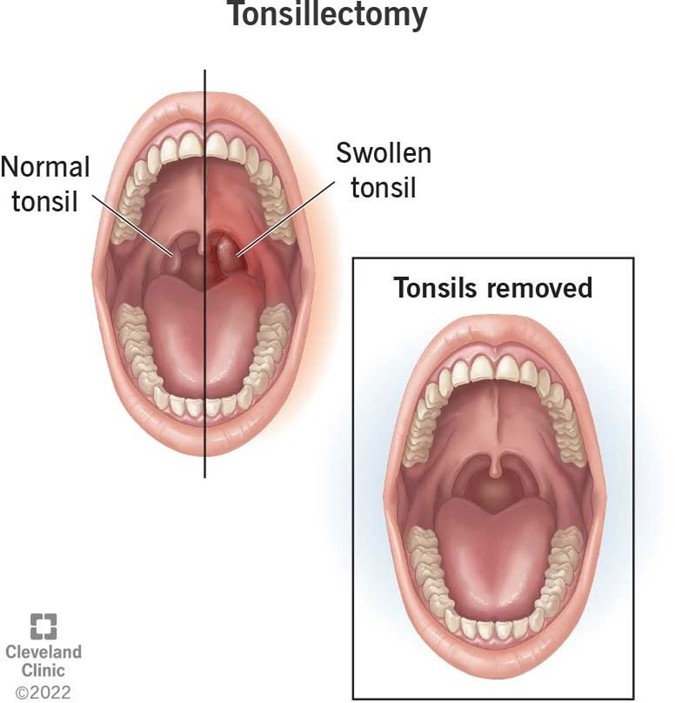
A nurse is caring for a child who is 2 hours postoperative following a tonsillectomy. Which of the following fluid items should the nurse offer the child at this time?
Cranberry juice
Crushed ice
Orange juice
Strawberry milkshake
The Correct Answer is B
Choice A: Cranberry juice is not a suitable fluid item to offer the child at this time, as it is acidic and can irritate the throat and cause pain or bleeding. Cranberry juice can also stain the surgical site and make it difficult to assess for signs of hemorrhage.
Choice B: Crushed ice is a suitable fluid item to offer the child at this time, as it is cold and can soothe the throat and
reduce swelling or inflammation. Crushed ice can also hydrate the child and prevent dehydration.
Choice C: Orange juice is not a suitable fluid item to offer the child at this time, as it is acidic and can irritate the throat and cause pain or bleeding. Orange juice can also interfere with the clotting process and increase the risk of hemorrhage.
Choice D: A strawberry milkshake is not a suitable fluid item to offer the child at this time, as it contains dairy products and can increase mucus production and cause coughing or gagging. A strawberry milkshake can also stain the surgical site and make it difficult to assess for signs of hemorrhage.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Choice A: Tachycardia is not a finding that indicates increased intracranial pressure, but rather a sign of shock, dehydration, or pain. Tachycardia is a fast heart rate, which is more than 160 beats per minute in infants. Tachycardia can occur when the body tries to compensate for low blood pressure, fluid loss, or tissue damage.
Choice B: Increased sleeping is a finding that indicates increased intracranial pressure, as it reflects altered level of consciousness, which is one of the earliest and most sensitive signs of increased intracranial pressure. Increased intracranial pressure can compress the brain tissue and affect its function and responsiveness. Increased sleeping can progress to lethargy, stupor, or coma.
Choice C: Brisk pupillary reaction to light is not a finding that indicates increased intracranial pressure, but rather a normal and expected response. A brisk pupillary reaction to light means that the pupils constrict quickly when exposed to bright light and dilate quickly when exposed to dim light. Brisk pupillary reaction to light indicates intact cranial nerve II (optic) and III (oculomotor).
Choice D: Depressed fontanels are not a finding that indicates increased intracranial pressure, but rather a sign of dehydration or malnutrition. Depressed fontanels are sunken or flat areas on the top or back of an infant's head where the skull bones have not yet fused together. Depressed fontanels can occur when there is insufficient fluid or tissue volume in the body.
Correct Answer is D
Explanation
Choice A: Allowing for imaginative play with peers without supervision is not an appropriate intervention for a child who has autism spectrum disorder, as it can cause frustration, anxiety, or isolation for the child. A child who has autism spectrum disorder may have difficulty with social skills, communication, and imagination, which can affect their ability to interact and play with others. The nurse should provide structured and supervised play activities that promote socialization and cooperation.
Choice B: Providing a completely unpredictable schedule that adjusts to the child's interests is not an appropriate intervention for a child who has autism spectrum disorder, as it can cause confusion, stress, or tantrums for the child. A child who has autism spectrum disorder may have difficulty with transitions, changes, and flexibility, which can affect their ability to cope and adapt to different situations. The nurse should provide a consistent and predictable schedule that follows a routine and gives clear expectations.
Choice C: Allowing for adjustment of rules to correlate with the child's behavior is not an appropriate intervention for a child who has autism spectrum disorder, as it can cause inconsistency, insecurity, or manipulation for the child. A child who has autism spectrum disorder may have difficulty understanding and following rules, which can affect their ability to behave and function appropriately. The nurse should provide firm and fair rules that are enforced consistently and respectfully.
Choice D: Establishing a reward system for positive behavior with prizes is an appropriate intervention for a child who has autism spectrum disorder, as it can provide motivation, reinforcement, and feedback for the child. A child who has autism spectrum disorder may have difficulty with learning and performing new skills, which can affect their ability to achieve and succeed. The nurse should provide a reward system that recognizes and rewards positive behavior with tangible or intangible prizes.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today