A nurse is discussing the differences between skeletal and skin traction with a newly licensed nurse. Which of the following statements by the newly licensed nurse indicates understanding?
Clients with skin traction have more mobility than those with skeletal traction.
Clients with skin traction have more discomfort than those with skeletal traction.
Skeletal traction is more appropriate than skin traction for reducing a fracture.
Skeletal traction has less risk for infection than skin traction.
The Correct Answer is C
Choice A reason:
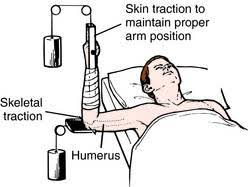
Skin traction is indeed less restrictive than skeletal traction, allowing for more mobility. It is applied using bandages or adhesive material to the skin, which can be removed or adjusted more easily than the pins or screws used in skeletal traction. This type of traction is typically used for short-term treatment before surgery or when the injury is less severe.
Choice B reason:
Discomfort levels can vary depending on the individual and the specific circumstances of the traction. However, skin traction is generally considered to be less painful than skeletal traction because it is less invasive and applies less force. Skeletal traction, which involves the insertion of pins or wires directly into the bone, is likely to cause more discomfort due to the invasive nature of the procedure.
Choice C reason:
Skeletal traction is more appropriate for reducing fractures, especially in cases where a greater force is needed to align the bones. It involves the surgical insertion of pins or wires directly into the bone, allowing for a stronger and more stable pull that is necessary for the realignment of complex fractures.
Choice D reason:
Skeletal traction carries a higher risk of infection compared to skin traction because it is more invasive. The insertion of pins or wires into the bone creates a potential entry point for bacteria, which can lead to infection at the site of insertion.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
Choice A Reason:
Administering antibiotics is a primary intervention for AGN when it is caused by a bacterial infection, such as post-streptococcal glomerulonephritis. Antibiotics help eliminate the infection and prevent further damage to the glomeruli.
Choice B Reason:
Encouraging increased fluid intake is not typically recommended for AGN, especially if the client has oliguria or edema, which are common in this condition. Fluid intake may need to be restricted to prevent fluid overload and worsening of hypertension.
Choice C Reason:
Frequent ambulation is not a priority intervention for AGN. While maintaining mobility is important, it does not directly address the renal inflammation or potential complications associated with AGN.
Choice D Reason:
Obtaining weight weekly is important for monitoring fluid status, but it is not the primary intervention. Daily weight measurements are more indicative of fluid retention or loss and are essential for closely monitoring the client's fluid balance.
Correct Answer is C
Explanation
Choice A reason:
Keeping artificial nails trimmed is a recommended practice in healthcare settings to maintain effective hand hygiene. Long nails can harbor bacteria and make it difficult to clean hands thoroughly. However, the CDC does not provide specific guidelines on the length of artificial nails for healthcare workers.
Choice B reason:
When caring for a client with Clostridium difficile, it is recommended to wash hands with soap and water rather than using alcohol-based hand rubs. Alcohol-based hand rubs are not effective against C. difficile spores. Therefore, thorough handwashing with soap and water is necessary to remove spores.
Choice C reason:
Chlorhexidine is an antiseptic agent that provides broad-spectrum antimicrobial activity and is recommended for hand hygiene in certain situations, such as before invasive procedures or for clients who are immunosuppressed. It is effective against a wide range of bacteria, viruses, and fungi, making it a suitable choice for immunocompromised patients to reduce the risk of infection.
Choice D reason:
The use of alcohol-based hand rubs before administering eye drops is not specifically recommended. While hand hygiene is essential before any contact with a patient, there is no particular preference for alcohol-based hand rubs in this context. The primary concern is to ensure that hands are clean to prevent contamination of the eye drops or the patient's eyes.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today