A nurse is developing an activity plan for a client. The nurse should recognize that which activity plan would best conserve the client's energy without compromising physical or mental health.
Scheduling energy-intensive activities at the time of day when the client has higher energy levels.
Scheduling all activities within a small block of time to allow the client a longer, uninterrupted rest period.
Scheduling toilet breaks before and after any other planned activity.
Scheduling the client's hygiene activities and limiting visitors.
The Correct Answer is A
Choice A reason: Scheduling energy-intensive activities at the time of day when the client has higher energy levels is the best activity plan for conserving the client's energy without compromising physical or mental health, as it allows the client to perform the tasks that require more effort and endurance when they feel more alert and capable. This can help the client to avoid fatigue, frustration, and injury, and to achieve their goals more effectively. The nurse should assess the client's individual preferences and patterns of energy fluctuation, and help them to prioritize and plan their activities accordingly.
Choice B reason: Scheduling all activities within a small block of time to allow the client a longer, uninterrupted rest period is not a good activity plan for conserving the client's energy without compromising physical or mental health, as it may cause the client to overexert themselves and deplete their energy reserves. This can lead to exhaustion, pain, and stress, and impair the client's recovery and quality of life. The nurse should advise the client to balance their activities with adequate rest periods throughout the day and to avoid doing too much or too little at once.
Choice C reason: Scheduling toilet breaks before and after any other planned activity is not a good activity plan for conserving the client's energy without compromising physical or mental health, as it may not be realistic or feasible for some clients. Some clients may have urinary or bowel problems that require them to use the toilet more frequently or urgently, such as incontinence, infection, or constipation. Forcing them to follow a rigid schedule may cause them discomfort, embarrassment, or complications. The nurse should assess the client's elimination needs and habits, and help them to manage their toileting needs in a comfortable and convenient way.
Choice D reason: Scheduling the client's hygiene activities and limiting visitors is not a good activity plan for conserving the client's energy without compromising physical or mental health, as it may neglect the client's social and emotional needs. Hygiene activities are important for maintaining the client's physical health and well-being, but they can also be tiring and challenging for some clients. Limiting visitors may reduce the noise and stimulation in the environment, but it can also isolate the client from their family and friends who can provide support and companionship. The nurse should assist the client with their hygiene needs as needed, and encourage them to interact with their visitors as tolerated.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Choice A: Collaborate with a physical therapist to develop programs for injured employees to return to work. This is incorrect because this is a tertiary prevention strategy, not a secondary prevention strategy. Tertiary prevention aims to restore function and prevent disability or complications after an injury or illness has occurred.
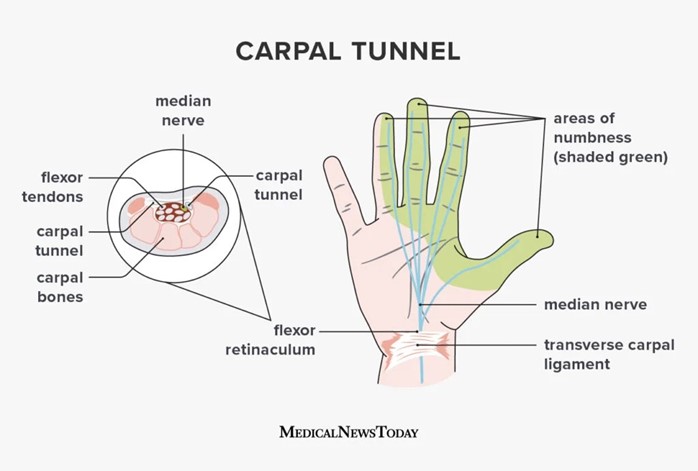
Choice B: Help plant workers identify signs of carpal tunnel syndrome. This is correct because this is a secondary prevention strategy. Secondary prevention aims to detect and treat health problems early before they become more serious or chronic. Carpal tunnel syndrome is a common occupational health problem that can cause pain, numbness, and weakness in the hand and wrist. Early identification and treatment can prevent permanent nerve damage and disability.
Choice C: Organize an influenza immunization campaign. This is incorrect because this is a primary prevention strategy, not a secondary prevention strategy. Primary prevention aims to prevent disease or injury from occurring in the first place, by reducing exposure or risk factors. Influenza immunization can protect plant workers from getting infected by the flu virus and reduce the spread of the disease.
Choice D: Teach plant workers about proper lifting techniques. This is incorrect because this is also a primary prevention strategy, not a secondary prevention strategy. Proper lifting techniques can prevent musculoskeletal injuries such as sprains, strains, and herniated discs, by avoiding excessive stress on the spine and joints.
Correct Answer is ["B","D","E"]
Explanation
Choice A reason: Initiating a plan of care for a client who is postoperative from an appendectomy is not a task that the RN should delegate to the LPN, as it requires nursing judgment, critical thinking, and assessment skills that are beyond the scope of practice of the LPN. The RN is responsible for developing, implementing, and evaluating the plan of care for each client based on their individual needs, preferences, and goals. The RN can delegate some aspects of the plan of care to the LPN, such as performing routine tasks or monitoring the client's status, but the RN must supervise and evaluate the LPN's performance.
Choice B reason: Administering a tap-water enema to a client who is preoperative is a task that the RN can delegate to the LPN, as it is a standardized procedure that does not require nursing judgment or assessment. The LPN has the knowledge and skills to perform this task safely and effectively, following the established policies and protocols of the facility. The RN should provide clear instructions and expectations to the LPN, such as the type, amount, and temperature of the solution, the position and comfort of the client, and the signs and symptoms to report. The RN should also verify that the LPN has completed the task and documented the outcome.
Choice C reason: Providing discharge instructions to a confused client's spouse is not a task that the RN should delegate to the LPN, as it involves teaching, counseling, and evaluating the client's and family's understanding and readiness for discharge. These are complex activities that require nursing judgment, communication skills, and evaluation skills that are beyond the scope of practice of the LPN. The RN is responsible for ensuring that the client and family receive adequate information and education about the client's condition, treatment, medications, follow-up care, and community resources. The RN can delegate some aspects of discharge planning to the LPN, such as collecting data or providing reinforcement of teaching, but the RN must supervise and evaluate the LPN's performance.
Choice D reason: Catheterizing a client who has not voided in 8 hours is a task that the RN can delegate to the LPN, as it is a standardized procedure that does not require nursing judgment or assessment. The LPN has the knowledge and skills to perform this task safely and effectively, following the established policies and protocols of the facility. The RN should provide clear instructions and expectations to the LPN, such as the type and size of the catheter, the sterile technique, and the urine output measurement. The RN should also verify that the LPN has completed the task and documented the outcome.
Choice E reason: Obtaining vital signs from a client who is 6 hours postoperative is a task that the RN can delegate to the LPN, as it is a routine task that does not require nursing judgment or assessment. The LPN has the knowledge and skills to perform this task safely and effectively, using appropriate equipment and techniques. The RN should provide clear instructions and expectations to the LPN, such as the frequency and parameters of vital signs monitoring. The RN should also verify that the LPN has completed the task and documented the outcome.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today