A nurse is contributing to the plan of care for a client who has Parkinson's disease. Which of the following interventions should the nurse plan to include?
Restrict the client's fluid intake
Keep suction equipment at the client's bedside
Instruct the client to look down when ambulating
Position the client supine after eating
The Correct Answer is B
b. Keep suction equipment at the client's bedside.
The nurse should plan to include keeping suction equipment at the client's bedside as an intervention for a client with Parkinson's disease. Parkinson's disease can cause dysphagia (difficulty swallowing) and an increased risk of aspiration. Having suction equipment readily available allows for prompt intervention in case of choking or aspiration episodes, ensuring the client's safety.
Explanation for the other options:
a. Restrict the client's fluid intake: Restricting the client's fluid intake is not typically indicated in the care of a client with Parkinson's disease. Adequate hydration is important for overall health and well-being. However, specific fluid restrictions may be necessary in certain situations, such as if the client has coexisting conditions like heart failure or kidney disease, which should be assessed and determined by the healthcare provider.
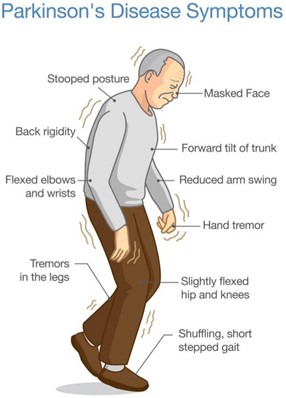
c. Instruct the client to look down when ambulating: In Parkinson's disease, individuals often experience a forward-flexed posture and a shuffling gait. Instructing the client to look down when ambulating is not an appropriate intervention. Instead, the nurse should encourage the client to maintain an upright posture, take smaller steps, and focus on taking deliberate and controlled movements to promote stability and reduce the risk of falls.
d. Position the client supine after eating: Positioning the client supine after eating is not recommended for a client with Parkinson's disease. This position can increase the risk of aspiration, as it may promote reflux and regurgitation of stomach contents. Instead, the nurse should advise the client to maintain an upright position, such as sitting in a chair or using a recliner with appropriate head support, to aid digestion and reduce the risk of aspiration.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
d. Apply the dressing loosely over the incision.
Explanation:
The correct answer is d. Apply the dressing loosely over the incision.
When caring for an older adult client, it is important for the nurse to be sensitive to age-related changes and promote their comfort and well-being. Applying the dressing loosely over the incision allows for beter circulation and ventilation, which can help prevent complications such as skin breakdown and infection.
Option a is not the correct answer. Asking the client to help with the dressing change may not be appropriate, as postoperative clients, especially older adults, may have limited mobility or dexterity. It is the nurse's responsibility to provide the necessary care and support during the dressing change.
Option b is not the correct answer. Waiting for the client to approach the nurse for assistance may lead to delays in care and could potentially compromise the client's healing process. The nurse should proactively assess the client's needs and provide appropriate care.
Option c is not the correct answer. Using paper tape for securing the new dressing does not specifically address sensitivity to age-related changes. While paper tape may be gentle on the skin, it is not the primary consideration in this situation.
By applying the dressing loosely over the incision, the nurse demonstrates sensitivity to age-related changes and promotes the client's comfort and optimal healing. This approach takes into account the potential for decreased skin elasticity and fragility in older adults, allowing for proper circulation and reducing the risk of complications.
Correct Answer is C
Explanation
The charge nurse should remind the newly licensed nurse that the client has a right to refuse medication. It is important for healthcare providers to respect the autonomy and rights of their clients, including the right to refuse treatment.
Option a is incorrect because it may not be appropriate for the family to persuade the client to take medication against their wishes.
Option b is incorrect because delivering medication intramuscularly against the client's wishes would violate their right to refuse treatment.
Option d is incorrect because inquiring about compatible foods with the pharmacy would not address the issue of the client's right to refuse medication.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today