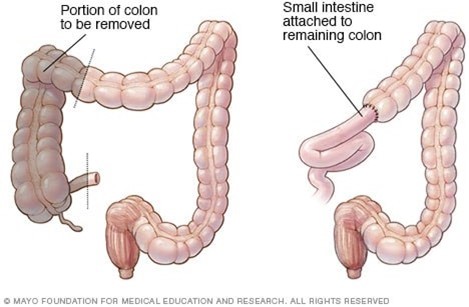
A nurse is caring for a client who is postoperative following a hemicolectomy. Which of the following is a subjective indication that the client needs PRN pain medication?
The client's heart rate is 110/min.
The client is guarding their abdominal incision.
The client exhibits facial grimacing.
The client reports pain.
The Correct Answer is D
The subjective indication that the client needs PRN (as needed) pain medication is when the client reports pain. Pain is a subjective experience, and it is essential to address the client's self-reported pain level and provide appropriate pain management.
Explanation for the other options:
a) The client's heart rate is 110/min: An increased heart rate can be an objective indication of pain, but it is not a subjective indication. Subjective indications are based on the client's self-report or personal experiences.
b) The client is guarding their abdominal incision: Guarding the abdominal incision may suggest discomfort or pain, but it is an objective indication that can be observed by the nurse. Subjective indications focus on the client's self-report.
c) The client exhibits facial grimacing: Facial grimacing can be an objective indication of pain, but it is not a subjective indication. Again, subjective indications are based on the client's self-report or personal experiences.
In this scenario, the most reliable and appropriate indication for administering PRN pain medication is when the client reports pain, as this acknowledges the client's own perception of their pain level.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
B. The school-age sister views death as being a type of temporary sleep:
This response aligns with developmental stages. School-age children (around ages 5-9) often have a more concrete understanding of death but may still see it as reversible or temporary, such as a long sleep. This is a normal way children in this age group might conceptualize death before they fully understand its permanence. It's common for them to express the idea that the person who has died will wake up or return in some way, as their cognitive understanding is still developing.
Correct Answer is B
Explanation
b. "Everyone who lives in the home will need medication."
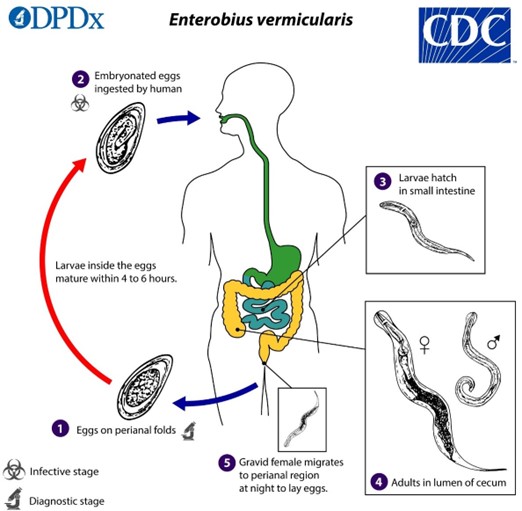
The nurse should inform the guardian that everyone who lives in the home will need medication when reinforcing teaching about enterobiasis. Enterobiasis, also known as pinworm infection, is highly contagious, and it can easily spread from person to person within the household. Treating only the affected individual may not be sufficient to eliminate the infection completely, as other household members may also be infected or at risk of reinfection.
Explanation for the other options:
a. "One dose of medication is all that will be necessary." Enterobiasis is typically treated with a medication regimen that involves taking multiple doses over a period of time. This is to ensure that all stages of the pinworm life cycle are targeted and eradicated. A single dose is usually not sufficient to eliminate the infection completely.
c. "Allow the child to take tub baths instead of showers." The choice of tub baths or showers does not directly impact the treatment or prevention of enterobiasis. Both methods of bathing can be used, but it is important to maintain good hygiene practices, such as regular handwashing and proper cleaning of the perianal area, to reduce the risk of reinfection.
d. "Wash all clothes and bed linens in cold water." While proper hygiene practices and laundering of clothes and bed linens are important in preventing the spread of enterobiasis, using cold water alone may not be sufficient. Washing clothes and bed linens in hot water (at a temperature of at least 60°C or 140°F) is recommended to kill any pinworm eggs that may be present.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today