A nurse is collecting data from a client who has obstruction and inflammation of the common bile duct due to cholelithiasis. Which of the following findings is expected for this condition?
Faty stools
Ecchymosis of the extremities
Straw-colored urine
Tenderness in the left upper abdomen
The Correct Answer is A
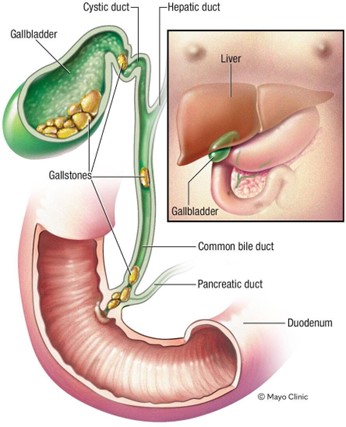
Choice A: Faty stools. This is a finding that is expected for a client who has obstruction and inflammation of the common bile duct due to cholelithiasis, which is the presence of gallstones in the gallbladder or bile ducts. The common bile duct carries bile from the liver and gallbladder to the duodenum, where it helps digest fats. If the common bile duct is obstructed by a gallstone, bile cannot reach the duodenum and fats cannot be properly absorbed. This results in fatty stools, which are also known as steatorrhea. Fatty stools are pale, bulky, greasy, and foul-smelling.
Choice B: Ecchymosis of the extremities. This is not a finding that is expected for a client who has obstruction and inflammation of the common bile duct due to cholelithiasis. Ecchymosis of the extremities is a sign of bleeding under the skin, which can be caused by trauma, coagulation disorders, or medications. It is not related to bile duct obstruction or gallstones.
Choice C: Straw-colored urine. This is not a finding that is expected for a client who has obstruction and inflammation of the common bile duct due to cholelithiasis. Straw-coloured urine is a normal colour of urine, which indicates adequate hydration and kidney function. It is not affected by bile duct obstruction or gallstones.
Choice D: Tenderness in the left upper abdomen. This is not a finding that is expected for a client who has obstruction and inflammation of the common bile duct due to cholelithiasis. Tenderness in the left upper abdomen is a sign of splenomegaly, which is an enlargement of the spleen due to infection, inflammation, or cancer. It is not related to bile duct obstruction or gallstones.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
Choice A: Implement neutropenia isolation. This is not an action that the nurse should take for a client who has developed a Clostridium difficile infection. Neutropenia isolation is a type of protective isolation that is used for
clients who have low white blood cell counts and are at risk of infection from others. It is not indicated for clients who have Clostridium difficile infection, which is not transmited through the air.
Choice B: Use alcohol hand sanitizer following client care. This is not an action that the nurse should take for a client who has developed a Clostridium difficile infection. Alcohol hand sanitizer is ineffective against Clostridium difficile spores and can increase the risk of transmission. The nurse should wash their hands with soap and water, which can remove the spores from the skin.
Choice C: Monitor the client for manifestations of fluid overload. This is not an action that the nurse should take for a client who has developed a Clostridium difficile infection. Fluid overload is a condition that occurs when the body retains excess fluid and causes symptoms such as edema, dyspnea, and hypertension. It is not related to Clostridium difficile infection, which can cause fluid loss due to diarrhea and dehydration. The nurse should monitor the client for manifestations of fluid deficit, such as dry mucous membranes, tachycardia, and hypotension.
Choice D: Disinfect equipment with bleach solution. This is an action that the nurse should take for a client who has developed a Clostridium difficile infection, which is a bacterial infection that causes severe diarrhea and inflammation of the colon. Clostridium difficile spores are resistant to most disinfectants and can survive on surfaces for a long time. The nurse should disinfect equipment with bleach solution, which can kill the spores and prevent transmission.
Correct Answer is D
Explanation
Choice A: Measure the tube for insertion from the tip of the nose to the umbilicus. This is not an intervention that the nurse should take when inserting a nasogastric tube. The nurse should measure the tube for insertion from the tip of the nose to the earlobe and then to the xiphoid process, which is a more accurate way of estimating the length of the tube needed to reach the stomach.
Choice B: Place the client in a supine position. This is not an intervention that the nurse should take when inserting a nasogastric tube. The nurse should place the client in a high-Fowler’s position, which is a position with the head of the bed elevated to 90 degrees. This position can prevent aspiration, promote breathing, and allow gravity to assist with the insertion of the tube.
Choice C: Withdraw the tube if the client gags during insertion. This is not an intervention that the nurse should take when inserting a nasogastric tube. The nurse should not withdraw the tube if the client gags during insertion, as this can cause trauma to the nasal or pharyngeal mucosa and increase discomfort. The nurse should pause and allow the client to rest and breathe until gagging subsides, then resume insertion. The nurse should also provide reassurance and encouragement to the client throughout the procedure.
Choice D: Instruct the client to place his chin to his chest and swallow. This is an intervention that the nurse should take when inserting a nasogastric tube, which is a flexible tube that is inserted through the nose and into the stomach. The nurse should instruct the client to place his chin to his chest and swallow as the tube passes through the pharynx and into the esophagus. This can facilitate the insertion of the tube and prevent it from entering the trachea or causing injury to the nasal or pharyngeal mucosa.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today