A nurse is caring for a client who is postoperative and has a history of Addison’s disease. For which of the following manifestations should the nurse monitor?
Hypernatremia
Bradycardia
Hypotension
Hypokalemia
The Correct Answer is C
Choice A: Hypernatremia. This is not a manifestation that the nurse should monitor for in a client who is postoperative and has a history of Addison’s disease. Hypernatremia is a high level of sodium in the blood, which can be caused by dehydration, excessive sodium intake, or kidney dysfunction. It is not related to Addison’s disease or cortisol and aldosterone levels.
Choice B: Bradycardia. This is not a manifestation that the nurse should monitor for in a client who is postoperative and has a history of Addison’s disease. Bradycardia is a slow heart rate, which can be caused by vagal stimulation, medication side effects, or cardiac disorders. It is not related to Addison’s disease or cortisol and aldosterone levels.
Choice C: Hypotension. This is a manifestation that the nurse should monitor for in a client who is postoperative and has a history of Addison’s disease, which is a condition that occurs when the adrenal glands do not produce enough cortisol and aldosterone. Cortisol is a hormone that regulates the metabolism of carbohydrates, proteins, and fats, and helps the body cope with stress. Aldosterone is a hormone that regulates the balance of sodium and potassium in the blood and fluid volume. Addison’s disease can cause hypotension, which is a low blood pressure, due to decreased aldosterone production and fluid loss.
Choice D: Hypokalemia. This is not a manifestation that the nurse should monitor for in a client who is postoperative and has a history of Addison’s disease. Hypokalemia is a low level of potassium in the blood, which can be caused by diuretics, vomiting, diarrhea, or alkalosis. It is not related to Addison’s disease or cortisol and aldosterone levels.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
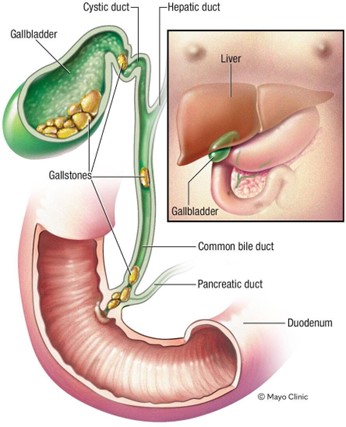
Choice A: Faty stools. This is a finding that is expected for a client who has obstruction and inflammation of the common bile duct due to cholelithiasis, which is the presence of gallstones in the gallbladder or bile ducts. The common bile duct carries bile from the liver and gallbladder to the duodenum, where it helps digest fats. If the common bile duct is obstructed by a gallstone, bile cannot reach the duodenum and fats cannot be properly absorbed. This results in fatty stools, which are also known as steatorrhea. Fatty stools are pale, bulky, greasy, and foul-smelling.
Choice B: Ecchymosis of the extremities. This is not a finding that is expected for a client who has obstruction and inflammation of the common bile duct due to cholelithiasis. Ecchymosis of the extremities is a sign of bleeding under the skin, which can be caused by trauma, coagulation disorders, or medications. It is not related to bile duct obstruction or gallstones.
Choice C: Straw-colored urine. This is not a finding that is expected for a client who has obstruction and inflammation of the common bile duct due to cholelithiasis. Straw-coloured urine is a normal colour of urine, which indicates adequate hydration and kidney function. It is not affected by bile duct obstruction or gallstones.
Choice D: Tenderness in the left upper abdomen. This is not a finding that is expected for a client who has obstruction and inflammation of the common bile duct due to cholelithiasis. Tenderness in the left upper abdomen is a sign of splenomegaly, which is an enlargement of the spleen due to infection, inflammation, or cancer. It is not related to bile duct obstruction or gallstones.
Correct Answer is D
Explanation
Choice A: Peri-umbilical area. This is not an area that the nurse should inspect to monitor for the presence of jaundice in a client who is African American and has cholecystitis. The peri-umbilical area is the area around the navel, which is part of the skin. The skin can show jaundice, but it may be difficult to detect in clients with dark skin tones.
Choice B: Nail beds. This is not an area that the nurse should inspect to monitor for the presence of jaundice in a client who is African American and has cholecystitis. The nail beds are part of the skin that can show jaundice, but they may also be affected by other factors such as anemia, cyanosis, or nail polish.
Choice C: Webbed areas of the fingers. This is not an area that the nurse should inspect to monitor for the presence of jaundice in a client who is African American and has cholecystitis. The webbed areas of the fingers are part of the skin that can show jaundice, but they may also be influenced by other factors such as temperature, circulation, or pressure.
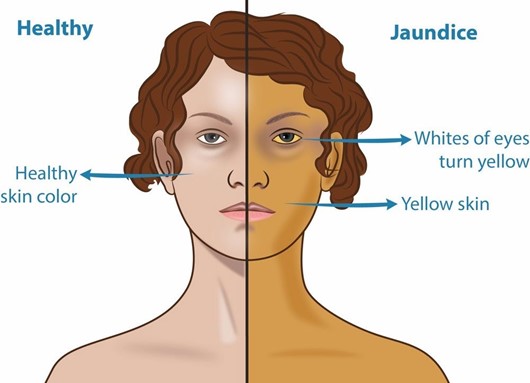
Choice D: Hard palate. This is an area that the nurse should inspect to monitor for the presence of jaundice in a client who is African American and has cholecystitis, which is an inflammation of the gallbladder. Jaundice is a yellowish discoloration of the skin and mucous membranes due to elevated bilirubin levels in the blood. Bilirubin is a pigment that is produced from the breakdown of red blood cells and is normally excreted in bile. If the gallbladder or bile ducts are inflamed or obstructed, bile cannot flow into the duodenum and bilirubin accumulates in the blood and tissues. The hard palate is a part of the oral mucosa that can show jaundice, especially in clients with dark skin tones.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today