The nurse is caring for a client who has a bowel obstruction and a new prescription for the insertion of a nasogastric tube. Which of the following interventions should the nurse take when inserting the nasogastric tube?
Measure the tube for insertion from the tip of the nose to the umbilicus.
Place the client in a supine position.
Withdraw the tube if the client gags during insertion.
Instruct the client to place his chin to his chest and swallow.
The Correct Answer is D
Choice A: Measure the tube for insertion from the tip of the nose to the umbilicus. This is not an intervention that the nurse should take when inserting a nasogastric tube. The nurse should measure the tube for insertion from the tip of the nose to the earlobe and then to the xiphoid process, which is a more accurate way of estimating the length of the tube needed to reach the stomach.
Choice B: Place the client in a supine position. This is not an intervention that the nurse should take when inserting a nasogastric tube. The nurse should place the client in a high-Fowler’s position, which is a position with the head of the bed elevated to 90 degrees. This position can prevent aspiration, promote breathing, and allow gravity to assist with the insertion of the tube.
Choice C: Withdraw the tube if the client gags during insertion. This is not an intervention that the nurse should take when inserting a nasogastric tube. The nurse should not withdraw the tube if the client gags during insertion, as this can cause trauma to the nasal or pharyngeal mucosa and increase discomfort. The nurse should pause and allow the client to rest and breathe until gagging subsides, then resume insertion. The nurse should also provide reassurance and encouragement to the client throughout the procedure.
Choice D: Instruct the client to place his chin to his chest and swallow. This is an intervention that the nurse should take when inserting a nasogastric tube, which is a flexible tube that is inserted through the nose and into the stomach. The nurse should instruct the client to place his chin to his chest and swallow as the tube passes through the pharynx and into the esophagus. This can facilitate the insertion of the tube and prevent it from entering the trachea or causing injury to the nasal or pharyngeal mucosa.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
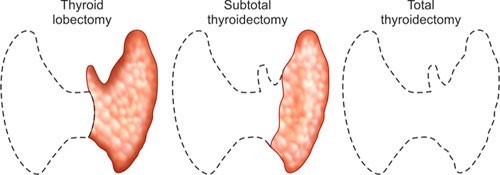
Choice A: Check for bleeding on the dressing at the back of the client’s neck. This is an implementation that the nurse should recommend for a client who is 4 hr postoperative from a subtotal thyroidectomy, which is a surgical removal of part of the thyroid gland. The nurse should check for bleeding on the dressing at the back of the client’s neck because this is where blood can pool and go unnoticed. Bleeding can cause hematoma, compression of the airway, and respiratory distress.
Choice B: Ensure that acetylcysteine IV is readily available. This is not an implementation that the nurse should recommend for a client who is 4 hr postoperative from a subtotal thyroidectomy. Acetylcysteine IV is an antidote for acetaminophen overdose, which can cause liver damage, but it is not related to thyroid surgery.
Choice C: Place the client in a side-lying position. This is not an implementation that the nurse should recommend for a client who is 4 hr postoperative from a subtotal thyroidectomy. The nurse should place the client in a semi-Fowler’s position, which is a position with the head of the bed elevated to 30 to 45 degrees. This position can facilitate breathing, reduce edema, and prevent aspiration.
Choice D: Check the client for asterixis. This is not an implementation that the nurse should recommend for a client who is 4 hr postoperative from a subtotal thyroidectomy. Asterixis is a sign of hepatic encephalopathy, which is a condition caused by liver failure, but it is not related to thyroid surgery.
Correct Answer is D
Explanation
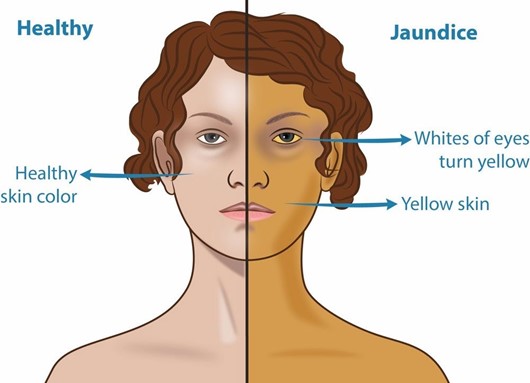
Choice A: Peri-umbilical area. This is not an area that the nurse should inspect to monitor for the presence of jaundice in a client who is African American and has cholecystitis. The peri-umbilical area is the area around the navel, which is part of the skin. The skin can show jaundice, but it may be difficult to detect in clients with dark skin tones.
Choice B: Nail beds. This is not an area that the nurse should inspect to monitor for the presence of jaundice in a client who is African American and has cholecystitis. The nail beds are part of the skin that can show jaundice, but they may also be affected by other factors such as anemia, cyanosis, or nail polish.
Choice C: Webbed areas of the fingers. This is not an area that the nurse should inspect to monitor for the presence of jaundice in a client who is African American and has cholecystitis. The webbed areas of the fingers are part of the skin that can show jaundice, but they may also be influenced by other factors such as temperature, circulation, or pressure.
Choice D: Hard palate. This is an area that the nurse should inspect to monitor for the presence of jaundice in a client who is African American and has cholecystitis, which is an inflammation of the gallbladder. Jaundice is a yellowish discoloration of the skin and mucous membranes due to elevated bilirubin levels in the blood. Bilirubin is a pigment that is produced from the breakdown of red blood cells and is normally excreted in bile. If the gallbladder or bile ducts are inflamed or obstructed, bile cannot flow into the duodenum and bilirubin accumulates in the blood and tissues. The hard palate is a part of the oral mucosa that can show jaundice, especially in clients with dark skin tones.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today