A nurse is collecting data from a 4-year-old child. Which of the following findings should the nurse expect?
Heart rate 110/min
Capillary refill greater than 3 seconds
Weight gain of 0.9 kg (2 lb) in a year
Respiratory rate 32/min
The Correct Answer is A
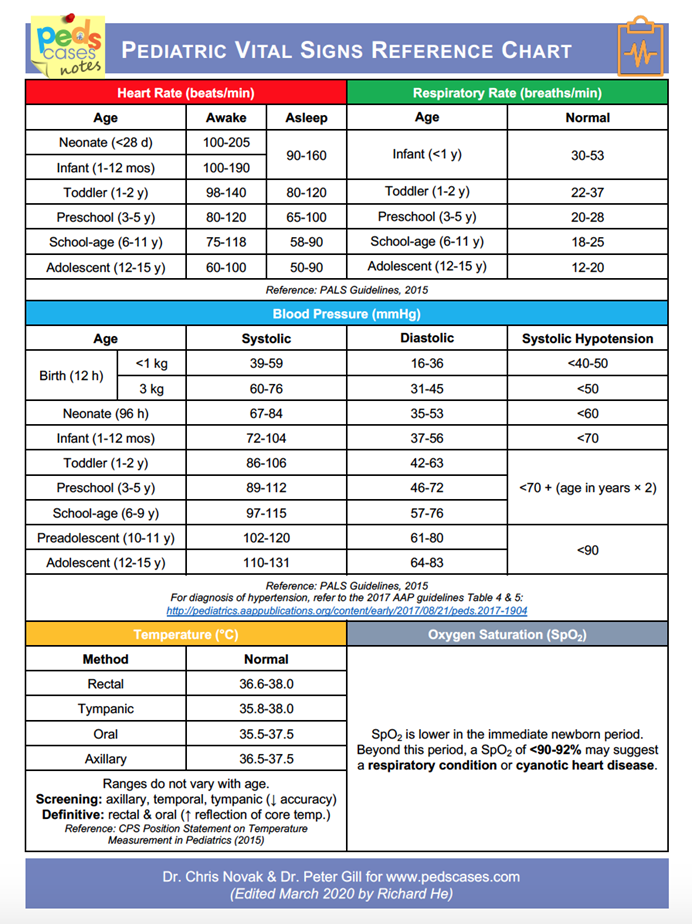
A. Heart rate 110/min: A heart rate of 110 beats per minute is within the normal range for a 4-year-old child. The typical heart rate for this age is between 80 to 120 beats per minute.
B. Capillary refill greater than 3 seconds: Capillary refill time should be less than 2 seconds in a healthy child. A refill time greater than 3 seconds may indicate poor perfusion or dehydration, which is abnormal.
C. Weight gain of 0.9 kg (2 lb) in a year: A weight gain of 2 pounds in a year is below the expected range for a 4-year-old. Children in this age group typically gain around 4-5 pounds per year as they grow.
D. Respiratory rate 32/min: The normal respiratory rate for a 4-year-old child is typically between 20 to 30 breaths per minute. A rate of 32/min is slightly elevated and may indicate respiratory distress or other issues.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
A. Restrain the toddler for 1 hr after the procedure: This is not necessary; the child should be monitored but not restrained.
B. Place the toddler in a side-lying, knee-chest position: This position helps to open the spaces between vertebrae, facilitating the lumbar puncture.
C. Ask another nurse to assist with holding the toddler in a prone position: The prone position is not appropriate for a lumbar puncture as it does not provide proper spinal alignment.
D. Swaddle the toddler in a warm blanket: While comforting, it is not relevant to the procedure itself.
Correct Answer is B
Explanation
A. 30 mL: Incorrect. This is far too high; it does not correspond to typical urine output.
B. 1 mL: Correct. It is a standard practice to equate 1 gram of wet diaper weight to 1 mL of urine, providing an accurate measure for fluid balance in infants.
C. 15 mL: Incorrect. This is too high for the given weight-to-volume ratio.
D. 5 mL: Incorrect. This is too high and does not match standard pediatric guidelines.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today