A nurse is collecting data for a client’s health history as well as physical examination.
Which of the following information should the nurse identify as a risk factor for type 2 diabetes mellitus?
History of exercise-induced asthma.
Age 35 years.
History of mumps.
BMI 32.2.
The Correct Answer is D
BMI 32.2.
A high body mass index (BMI) is a major risk factor for type 2 diabetes mellitus, as it indicates overweight or obesity.
Overweight or obesity can cause insulin resistance, which means the body cells do not respond well to insulin and cannot take up glucose from the blood. This leads to high blood sugar levels and diabetes.
Choice A is wrong because history of exercise-induced asthma is not a risk factor for type 2 diabetes mellitus.
Asthma is a respiratory condition that causes inflammation and narrowing of the airways, but it does not affect the metabolism of glucose or insulin.
Choice B is wrong because age 35 years is not a risk factor for type 2 diabetes mellitus.
Although the risk of diabetes increases with age, especially after 45 years, it can also occur in younger people.
Age alone is not enough to cause diabetes.
Choice C is wrong because history of mumps is not a risk factor for type 2 diabetes mellitus.
Mumps is a viral infection that affects the salivary glands, but it does not damage the pancreas or impair insulin production.
Some other risk factors for type 2 diabetes mellitus are family history, race or ethnicity, physical inactivity, prediabetes, gestational diabetes, polycystic ovarian syndrome, and smoking.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
The indirect Coombs test is used to detect antibodies against foreign red blood cells in the maternal serum. This test can help identify maternal-fetal blood incompatibility, which can cause hemolytic disease of the newborn.
Choice A is wrong because homocysteine is a type of amino acid and is not related to blood compatibility.
Choice C is incorrect because erythropoietin is a hormone that regulates red blood cell production and is not a specific test for detecting maternal-fetal blood incompatibility.
Choice D is not the correct answer as aPTT (activated partial thromboplastin time) is a test used to evaluate blood clotting factors and is not directly related to monitoring maternal-fetal blood incompatibility.
Correct Answer is B
Explanation
Obturator.
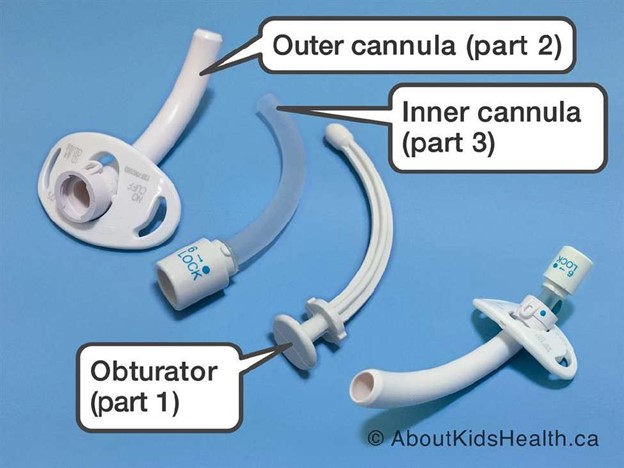
An obturator is a device that is inserted into the tracheostomy tube to guide it through the stoma and prevent tissue damage. It should be removed after the tube is inserted and kept near the bedside in case of accidental decannulation.
Choice A is wrong because povidone-iodine is an antiseptic solution that is not routinely used for tracheostomy care. It can cause skin irritation and damage to the mucous membranes.
Choice C is wrong because an irrigation set is not needed for a tracheostomy tube.
Irrigation can introduce bacteria and increase the risk of infection. It can also cause coughing and bleeding.
Choice D is wrong because hemostats are not used for a tracheostomy tube.
Hemostats are surgical instruments that are used to clamp blood vessels or tissues. They have no role in tracheostomy care.
Some other supplies that the nurse should place in the room are a trach tube the same size as the current tube and one size smaller, a portable suction machine with battery backup, and tubing that connects to the suction machine. Other supplies may include saline solution, syringes, gauze squares, gloves, a trachea tube brush, a waterproof drape, non-woven sponges, pipe cleaners, cotton tipped applicators, a T-drain sponge, twill tape, a trach holder, a speaking valve, a stoma cover, and a nebulizer.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today